

Cytotoxic therapy in acute myeloid leukemia: not quite dead yet
- PMID: 30504291
- PMCID: PMC6246033
- DOI: 10.1182/asheducation-2018.1.51
Cytotoxic therapy in acute myeloid leukemia: not quite dead yet
Abstract
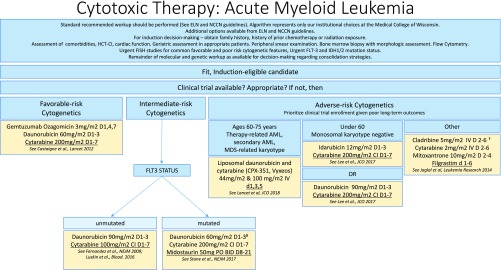
Given the recent approvals of new agents for acute myeloid leukemia (AML), a clinical trial pipeline stocked with novel therapies, and the rapid integration of imaginative approaches in diseases like acute lymphocytic leukemia and chronic lymphocytic leukemia, it is reasonable to ask whether treatment of AML might finally depart from the classical cytotoxic induction therapy that has been employed since the 1970s. However, for better or worse, in 2018, cytotoxic induction regimens remain the standard of care for most patients. Indeed, the future likely lies in combinations of therapies that act with a spectrum of mechanisms. Using a case-based format, this review will outline current treatment expectations for patients according to karyotypic risk and familiarize readers with the basis for common induction choices. Relapsed/refractory disease may be especially amenable to interventions with novel agents or clinical trials; however, there are still some patients who most benefit from intensive chemotherapy. This review will outline risk systems that help the practitioner identify those with the best chances for response and survival. Finally, clinical tools, including geriatric assessments and comorbidity calculators, may help clinicians recognize patients for whom disease risk and comorbidity tip the balance against classical chemotherapy, a frequent challenge for those who treat this devastating disease.
© 2018 by The American Society of Hematology. All rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: L.C.M. has served as a consultant on advisory boards for Celgene, Novartis, Jazz Pharmaceuticals, and Incyte, has consulted for Celgene, and receives research funding from Jazz Pharmaceuticals.
Figures
References
-
- Rowe JM. AML in 2017: Advances in clinical practice. Best Pract Res Clin Haematol. 2017;30(4):283-286. - PubMed
-
- DeVita VT Jr, Chu E. A history of cancer chemotherapy. Cancer Res. 2008;68(21):8643-8653. - PubMed
-
- Estey E, Gale RP. Acute myeloid leukemia therapy and the chosen people. Leukemia. 2017;31(2):269-271. - PubMed
-
- Dinmohamed AG, Visser O, van Norden Y, et al. . Treatment, trial participation and survival in adult acute myeloid leukemia: a population-based study in the Netherlands, 1989-2012. Leukemia. 2016;30(1):24-31. - PubMed
-
- Estey EH, Gale RP, Sekeres MA. New drugs in AML: uses and abuses. Leukemia. 2018;32(7):1479-1481. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical