

Clinical and laboratory diagnosis of TTP: an integrated approach
- PMID: 30504354
- PMCID: PMC6246034
- DOI: 10.1182/asheducation-2018.1.530
Clinical and laboratory diagnosis of TTP: an integrated approach
Abstract
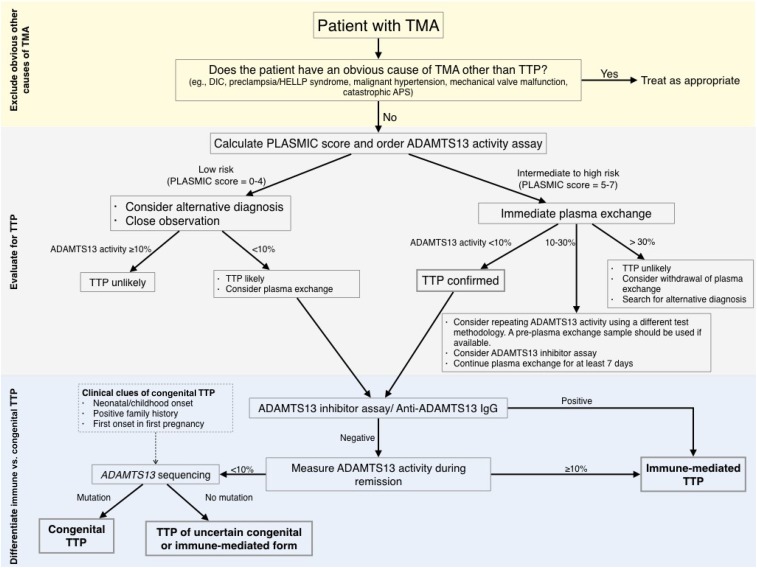
Thrombotic thrombocytopenia purpura (TTP) is a rare, life-threatening disease with an incidence of approximately 2 persons per million per year. It is characterized by severe deficiency of the von Willebrand cleaving protease, ADAMTS13 (a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13), leading to formation of platelet-rich thrombi in the microvasculature. Prompt initiation of appropriate therapy, particularly plasma exchange, may be life-saving. Diagnosis of TTP is challenging because of its diverse clinical manifestations, overlap in clinical presentation with other thrombotic microangiopathies, and limited availability of ADAMTS13 testing. Clinical prediction scores have been developed to estimate the pretest probability of severe ADAMTS13 deficiency and may be used as an adjunct to clinical judgment to guide initial management decisions. An ADAMTS13 activity level of less than 10% supports the diagnosis of TTP in appropriate clinical contexts, but many centers do not offer testing in-house and must send out the test to a reference laboratory with a turnaround time of several days. In such instances, initial management decisions must be made without the benefit of laboratory testing. In patients with TTP, inhibitor tests may be useful for distinguishing immune-mediated from congenital TTP. In this article, we review the epidemiology, natural history, and clinical presentation of TTP and laboratory assays for TTP including ADAMTS13 activity and inhibitor assays. We also describe an evidence-based approach to the evaluation of a patient with suspected TTP that integrates clinical and laboratory assessment.
© 2018 by The American Society of Hematology. All rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: A.C. has received research funding from Alexion, Bayer, Bioverativ, Novo Nordisk, Pfizer, Shire, Spark, and Syntimmune and has consulted for Genzyme, Kedrion, and Synergy. T.C. declares no competing financial interests.
Figures
References
-
- Scully M, Cataland S, Coppo P, et al. ; International Working Group for Thrombotic Thrombocytopenic Purpura. Consensus on the standardization of terminology in thrombotic thrombocytopenic purpura and related thrombotic microangiopathies. J Thromb Haemost. 2017;15(2):312-322. - PubMed
-
- Mariotte E, Azoulay E, Galicier L, et al. ; French Reference Center for Thrombotic Microangiopathies. Epidemiology and pathophysiology of adulthood-onset thrombotic microangiopathy with severe ADAMTS13 deficiency (thrombotic thrombocytopenic purpura): a cross-sectional analysis of the French national registry for thrombotic microangiopathy. Lancet Haematol. 2016;3(5):e237-e245. - PubMed
-
- Reese JA, Muthurajah DS, Kremer Hovinga JA, Vesely SK, Terrell DR, George JN. Children and adults with thrombotic thrombocytopenic purpura associated with severe, acquired Adamts13 deficiency: comparison of incidence, demographic and clinical features. Pediatr Blood Cancer. 2013;60(10):1676-1682. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical