

Comparison of bone texture between normal individuals and patients with Kashin-Beck disease from plain radiographs in knee
- PMID: 30504816
- PMCID: PMC6269488
- DOI: 10.1038/s41598-018-35552-8
Comparison of bone texture between normal individuals and patients with Kashin-Beck disease from plain radiographs in knee
Abstract
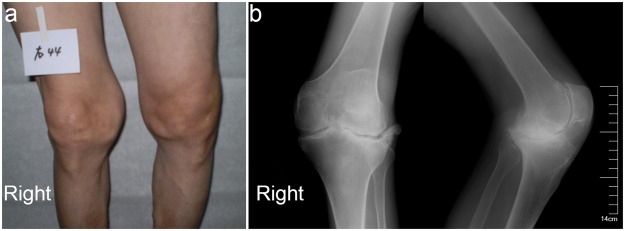
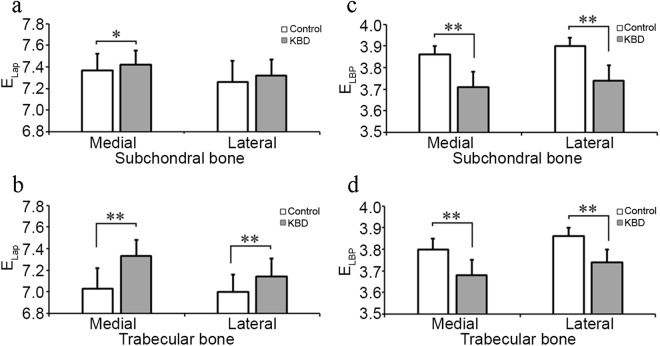
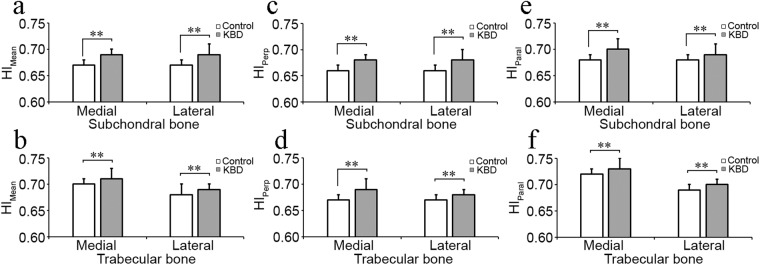
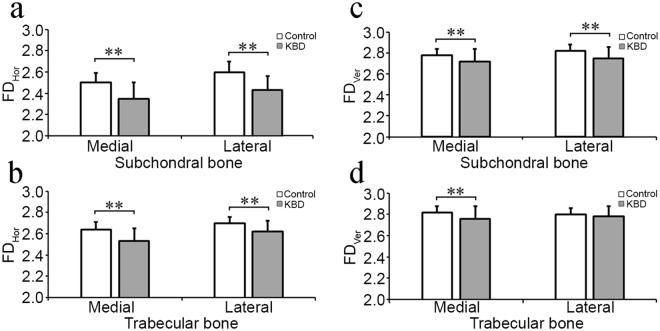
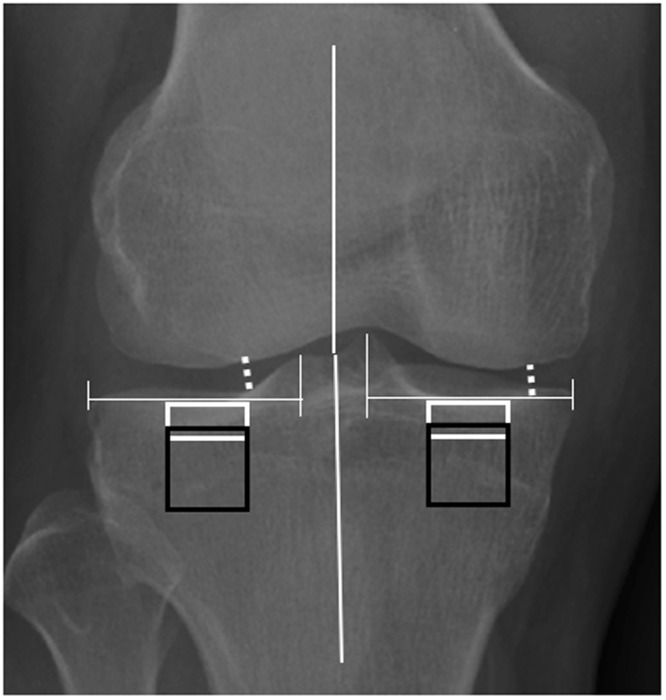
To compare tibial bone texture between Kashin-Beck disease (KBD) patients and normal individuals from plain radiographs using an advanced image analysis. Plain knee radiographs were obtained from KBD patients (n = 49) and age-matched healthy controls (n = 98). KBD were graded with diagnostic criteria WS/T 207-2010. The textural values related to bone structure from medial and lateral tibial subchondral and trabecular bones were evaluated using entropy of Laplacian-based image (ELap), entropy of local binary patterns (ELBP), homogeneity indices (HI) of local angles (HIMean, HIPerp and HIParal), and fractal dimensions from horizontal (FDHor) and vertical (FDVer) structures. KBD patients were shorter in height and lighter in weight, and their tibial width was wider than controls. Anatomical angle of KBD patients showed more genu valgus. Total KBD patients and subgroups had higher ELap, HIMean, HIPerp and HIParal in detected tibial subchondral and trabecular bones than controls, except ELap in lateral subchondral bone. ELBP, FDHor and FDVer from the detected tibial bone in KBD patients and subgroups were lower than controls, except FDVer in lateral trabecular bone. Our results indicate that micro-scale in bone texture in KBD-affected knees can be quantitatively examined from plain radiographs using an advanced image analysis.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Kraus, V. B. Rare Osteoarthritis: Ochronosis and Kashin-Beck Disease. In: Rheumatology, 6th edition, Eds M. C. Hochberg, A. J. Silman, J. S. Smolen, M. E. Weinblatt & M. H. Weisman (Mosby Elsevier, Philadelphia). Chapter 185, 1536–1540 (2014).
-
- Malaisse, F. & Mathieu, F. Big bone disease. A multidisciplinary approach of KBD in Tibet autonomous region (P.R. China). Les Presses agronomiques de Gembloux, A.S.B.L. 70–78 (2008).
Publication types
MeSH terms
Grants and funding
- 268378/Suomen Akatemia (Academy of Finland)/International
- 308165/Suomen Akatemia (Academy of Finland)/International
- 268378/Suomen Akatemia (Academy of Finland)/International
- 308165/Suomen Akatemia (Academy of Finland)/International
- 268378/Suomen Akatemia (Academy of Finland)/International
- 308165/Suomen Akatemia (Academy of Finland)/International
- 268378/Suomen Akatemia (Academy of Finland)/International
- 308165/Suomen Akatemia (Academy of Finland)/International
- 268378/Suomen Akatemia (Academy of Finland)/International
- 308165/Suomen Akatemia (Academy of Finland)/International
- 268378/Suomen Akatemia (Academy of Finland)/International
- 308165/Suomen Akatemia (Academy of Finland)/International
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
