

Wedged gel pad for bowel manipulation during MR-guided high-intensity focused ultrasound therapy to treat uterine fibroids: a case report
- PMID: 30505445
- PMCID: PMC6260726
- DOI: 10.1186/s40349-018-0116-4
Wedged gel pad for bowel manipulation during MR-guided high-intensity focused ultrasound therapy to treat uterine fibroids: a case report
Abstract
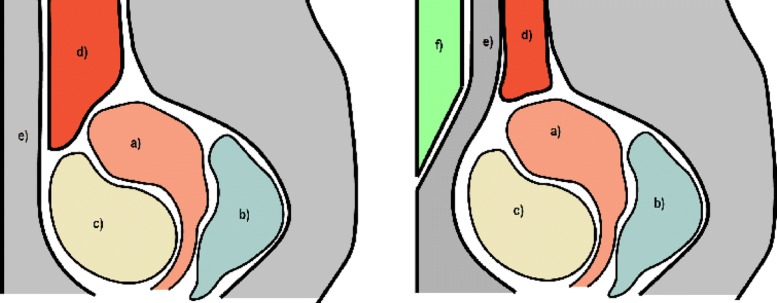
Background: Magnetic resonance guided high-intensity focused ultrasound (MR-HIFU) therapy is not feasible in all patients with uterine fibroids because of limiting anatomical factors such as scar tissue, bowel loops or other obstacles in the sonication path. These may prevent the treatment or limit the treatment window, and therefore, also the volume where HIFU therapy can be delivered. Bowel loops present a particular problem because of bowel gas bubbles and hard particles which may cause reflection or absorption of ultrasound energy, potentially leading to thermal damage and even bowel perforation. Most commonly used techniques for bowel repositioning are bladder and/or rectum filling but these are not always sufficient to reposition the bowel loops. With more efficient bowel repositioning technique, the number of eligible patients for MR-HIFU treatment could be increased, and therapy efficacy be improved in cases where bowel loops limit the treatment window.
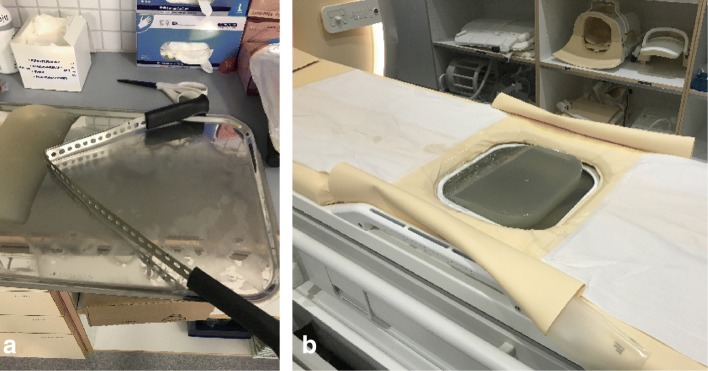
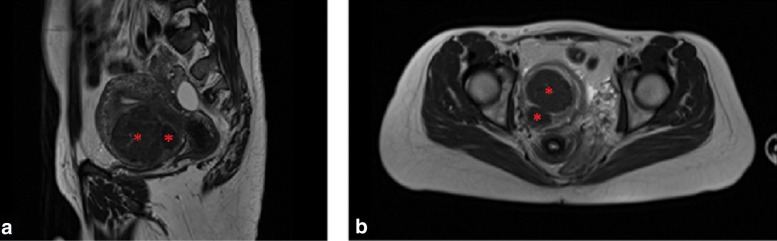
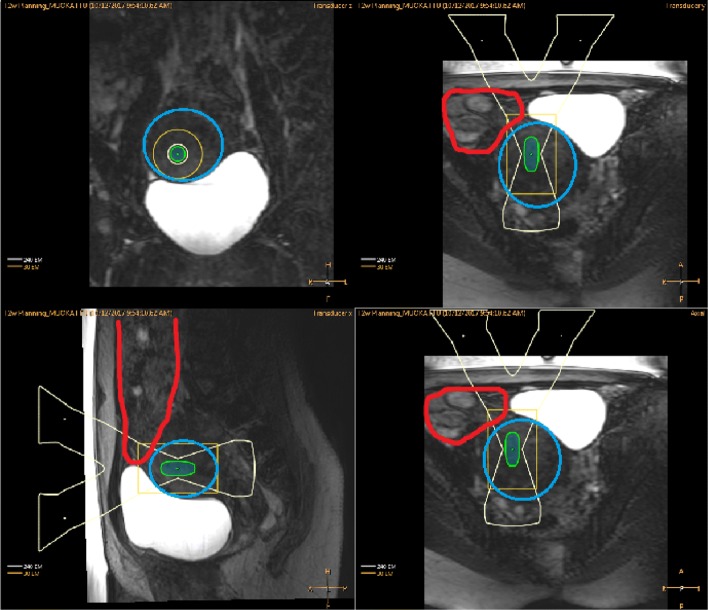
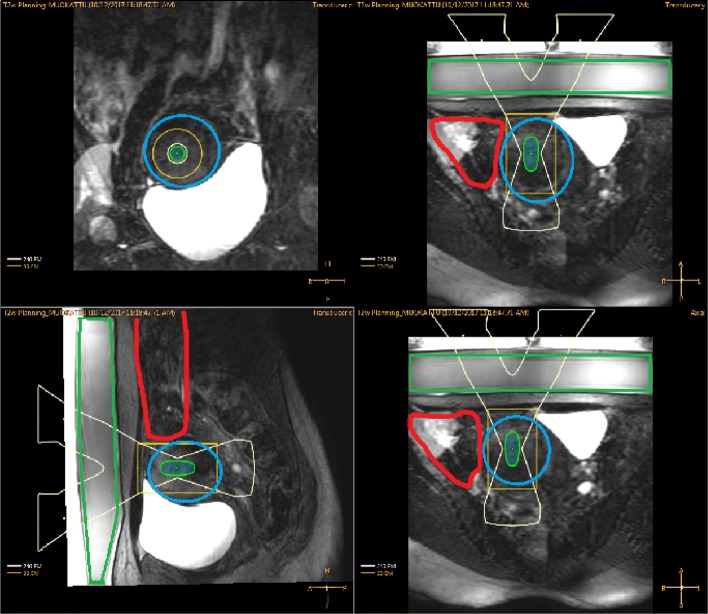
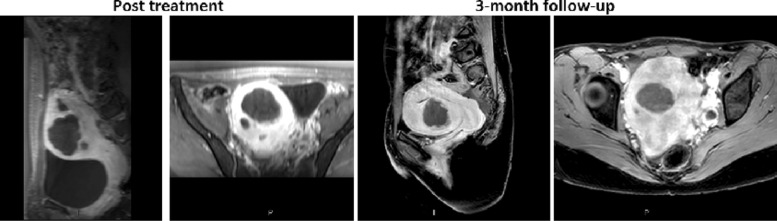
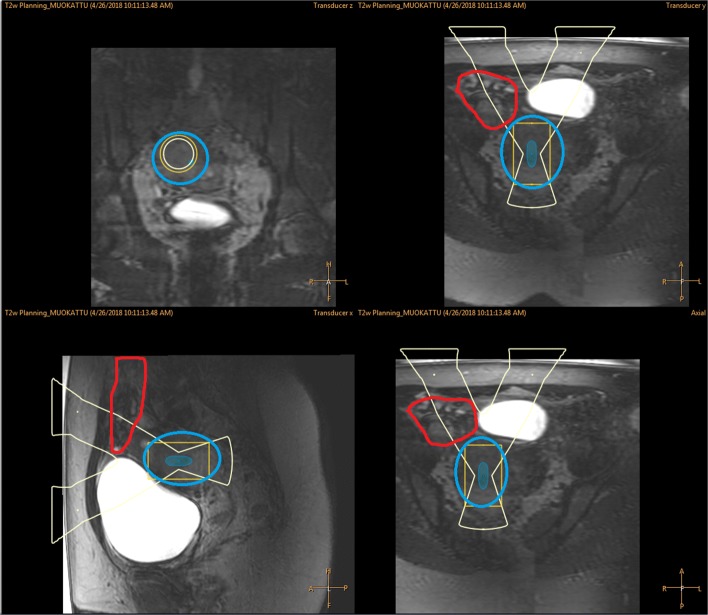
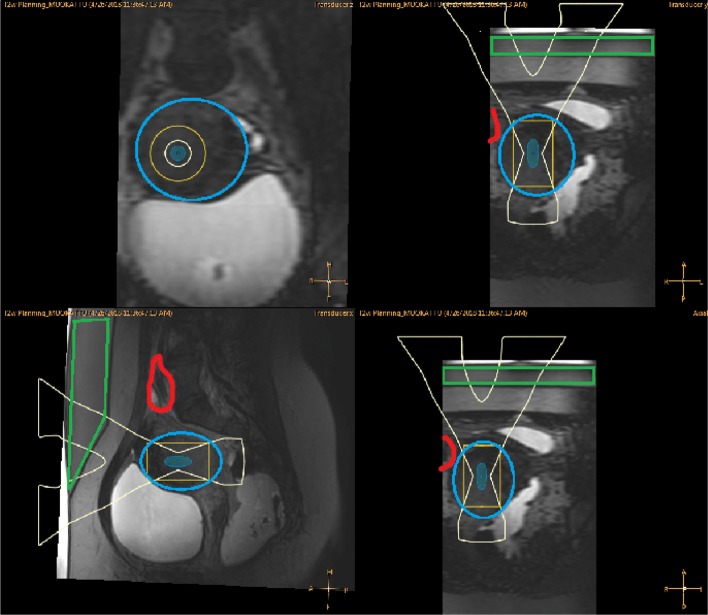
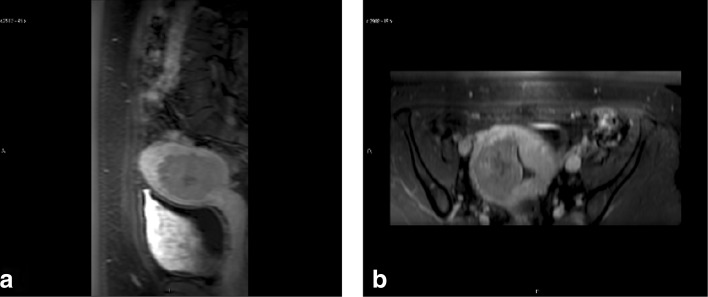
Case presentation: A wedged exterior gel pad was used in two patients presented with in total of four symptomatic fibroids undergoing MR-HIFU treatment when bladder and/or rectum filling was not sufficient to reposition the bowel loops. No severe adverse effects were observed in these cases. The non-perfused volume ratios (NPVs) immediately after treatment were 86% and 39% for the first patient, and 3% for the second patient.
Conclusions: Our preliminary experience suggests that the use of a wedged gel pad during MR-HIFU treatment could be an effective tool to manipulate the bowels in cases where the bladder and/or rectum filling is not sufficient to reposition the bowel loops. A wedged gel pad could also be used in other situations to achieve better treatment coverage to the uterine fibroid.
Keywords: Bowel repositioning; Gel pad; MR-guided high-intensity focused ultrasound; Uterine fibroid.
Conflict of interest statement
This case study was part of Treatment of Benign Uterine Disorders Using High Intensity Focused Ultrasound (MR-HIFU) trial (clinicaltrials.gov identifier NCT02914704). Local ethics committee approval was obtained from Ethics Committee, Hospital District of Southwest Finland for the protocol prior to study initiation.Consents for publication were obtained from all participants.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
LinkOut - more resources
Full Text Sources
