

Review
doi: 10.21037/jtd.2018.08.84.
Medical management of drug-sensitive active thoracic tuberculosis: the work-up, radiographic findings and treatment
Affiliations
- PMID: 30505525
- PMCID: PMC6218360
- DOI: 10.21037/jtd.2018.08.84
Item in Clipboard
Review
Medical management of drug-sensitive active thoracic tuberculosis: the work-up, radiographic findings and treatment
J Thorac Dis.
2018 Oct.
Abstract
Tuberculosis (TB) infection and disease have plagued human civilization across time and led to immeasurable morbidity and mortality. This review article focuses on the most currently available information regarding the diagnostic workup, radiologic presentation and treatment of drug-sensitive active TB. As discussed, if adequate resources and methods are available to diagnose, evaluate, and treat patients, drug sensitive TB is an imminently curable disease.
Keywords: Thoracic tuberculosis; diagnosis tuberculosis; radiology in tuberculosis; treatment tuberculosis.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
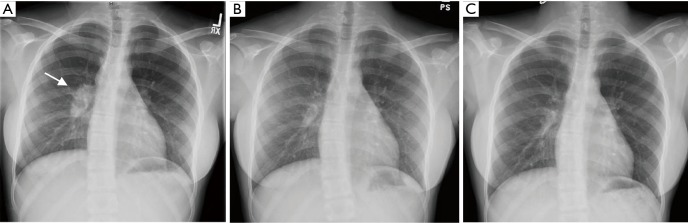
Radiographic improvement during the course of TB treatment in a 14-year-old Haitian girl. Upon presentation, the patient had an enlarged right hilar lymph node (arrow) (A) and more subtle nodular infiltrates in the right lower lobe on CT scan (not shown) which is typical of primary TB in a child. Sputum samples were negative for AFB, but the patient was started on empiric therapy with radiographic reassessment at 2 months (B) and 6 months (C) showing a gradual reduction in the lymph node size to normal allowing for classification as a clinical case. As discussed in the text, paradoxical enlargement in lymph nodes can occur with initiation of treatment and does not necessarily indicate treatment failure. TB, tuberculosis; AFB, acid fast bacilli.
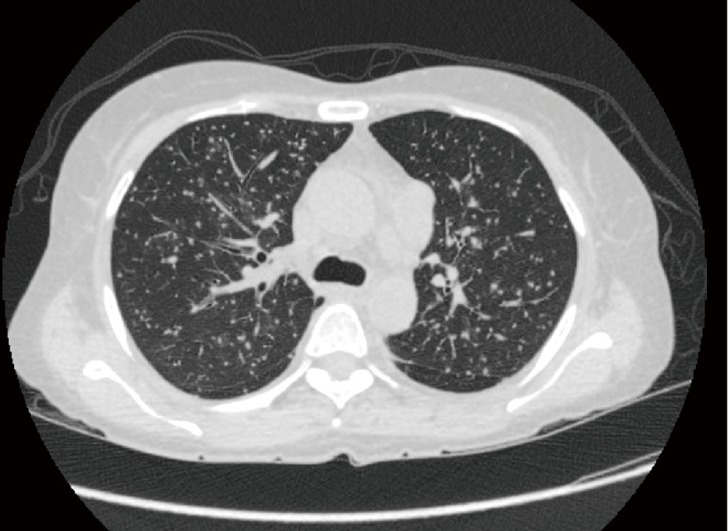
Computed tomography (CT) scan of a 46-year-old Vietnamese patient presenting with fever, fatigue and hypotension. Evident are innumerable small pulmonary nodules indicative of miliary TB. Despite the apparent extent of disease radiographically, confirming the diagnosis was difficult, with sputum samples negative because of the largely interstitial location of bacilli. Ultimately, a bronchoalveolar lavage was positive for MTB complex by PCR and the patient responded appropriately to therapy. This patient previously had 2 negative interferon gamma release assays, the last several months prior to presentation, suggesting this is an example of progressive primary TB. TB, tuberculosis; MTB, Mycobacterium tuberculosis.

Chest radiograph of a 54-year-old man presenting with cough for 4 months and 50-pound weight loss. There is a dense right upper lobe infiltrate with areas of cavitation (arrows) indicative of post-primary TB. He was AFB smear positive and culture positive for pan-sensitive bacilli. TB, tuberculosis; AFB, acid fast bacilli.
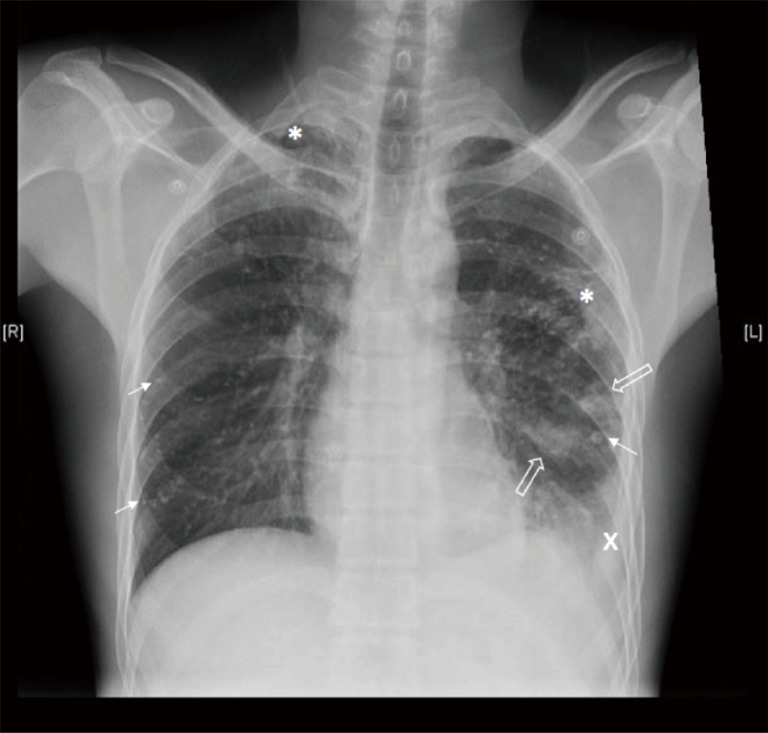
Post-primary active TB presenting with multiple concomitant radiographic findings in a 37-year-old man with active disease 20 years prior but incomplete therapy due to medication cost. Radiograph reveals multiple calcified nodules (solid arrows) and upper lobe fibrotic areas (*) typically seen after healed TB, but also the presence of a pleural effusion (x) and parenchymal infiltrates (open arrows), some of which were cavitary on CT. The patient was smear positive for AFB, grew pan-sensitive MTB, and the pleural effusion had an elevated adenosine deaminase but was sterile. As stated in the text and demonstrated by this case, imaging frequently cannot distinguish active and inactive disease. TB, tuberculosis; AFB, acid fast bacilli; MTB, Mycobacterium tuberculosis.
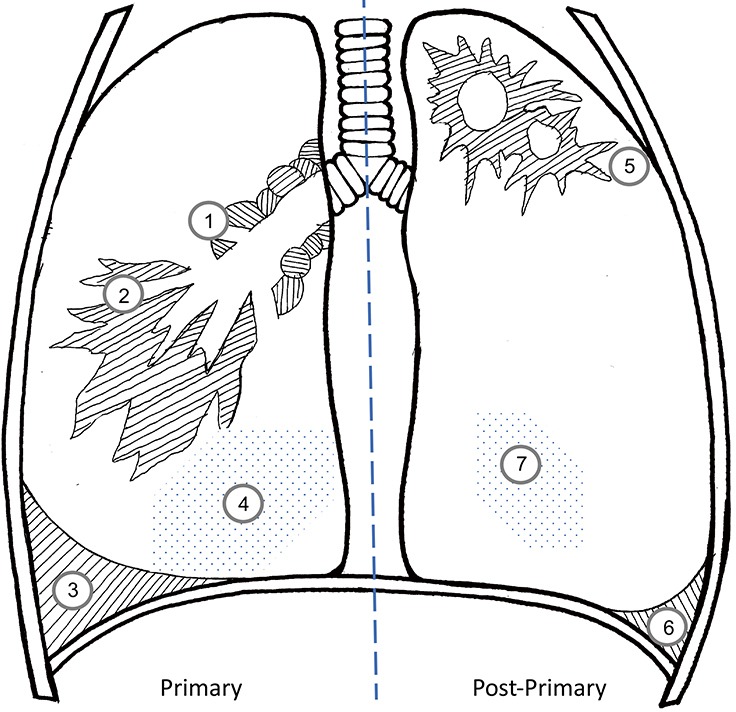
A summary of the typical radiographic manifestations in primary (left panel) and post-primary tuberculosis (right panel). Primary disease is largely characterized by mediastinal or hilar adenopathy which may cause airway compression (“1”) along with middle and lower lobe infiltrates (“2”) in adults. When unchecked, progressive primary disease leads to miliary spread (“4”). Pleural effusions (“3”) can be the sole manifestation of primary disease. In contrast, the parenchymal infiltrates of post-primary TB are usually apical and cavitary (“5”) with pleural effusions (“6”) and miliary spread (“7”) less common. Fibrotic changes may lead to volume loss with hilar or fissure displacement. Significant mediastinal adenopathy is uncommon in post-primary disease. While it is possible for several or all of these different radiographic findings to occur simultaneously in a single patient, this is less common and drawn in this manner for educational purposes.
References
-
- WHO. WHO Global Tuberculosis Report 2017. 2017. ISBN 978 92 4 156539 4.
-
- Lewinsohn DM, Leonard MK, Lobue PA, et al. Official American thoracic society/Infectious diseases society of America/Centers for disease control and prevention clinical practice guidelines: diagnosis of tuberculosis in adults and children. Clin Infect Dis 2017;64:111-5. 10.1093/cid/ciw778 - DOI - PMC - PubMed
-
- Mazurek GH, Jereb J, Vernon A, et al. Updated guidelines for using Interferon Gamma Release Assays to detect Mycobacterium tuberculosis infection - United States, 2010. MMWR Recomm Rep 2010;59:1-25. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials