

Review
doi: 10.21037/jtd.2018.08.85.
Surgical management of non-mycobacterial fungal infections
Affiliations
- PMID: 30505527
- PMCID: PMC6218364
- DOI: 10.21037/jtd.2018.08.85
Item in Clipboard
Review
Surgical management of non-mycobacterial fungal infections
J Thorac Dis.
2018 Oct.
Abstract
Fungal infections of the lung are common in endemic areas and in immunocompromised patients. Antifungal therapy is the cornerstone of medical therapy for most pulmonary fungi but surgery is an important adjunct in cases of complicated disease or resistant organisms. A multidisciplinary approach including pulmonary medicine, infectious disease, interventional radiology, and thoracic surgery is favored. This article reviews the surgical management of common fungal pulmonary infections and their sequelae.
Keywords: Fungus; cavitary; infection; lung; surgical management.
Conflict of interest statement
Conflicts of Interest: The author has no conflicts of interest to declare.
Figures

Surgical lung specimen from a patient with allergic bronchopulmonary aspergillosis (ABPA) and bronchiectasis. The specimen shows an aspergilloma within the area of saccular bronchiectasis.
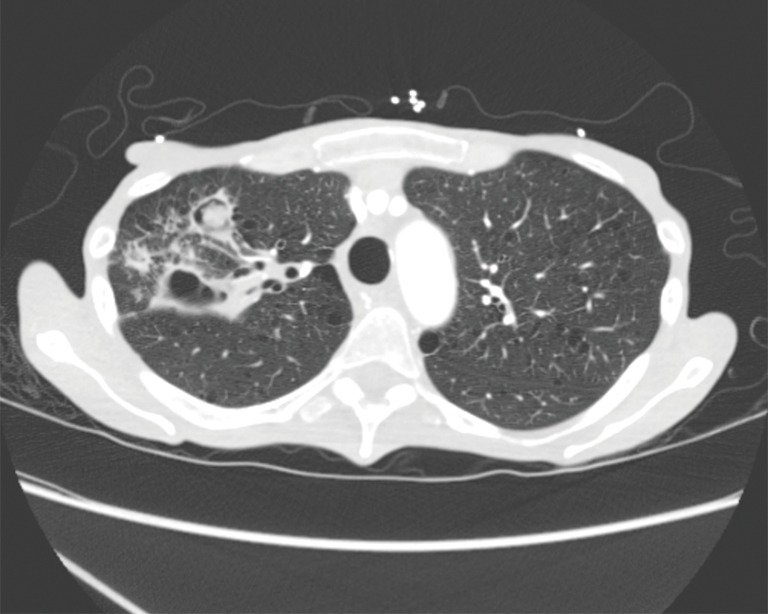
Complex right upper lobe aspergilloma in a cavitary lesion with destruction of adjacent lung parenchyma.
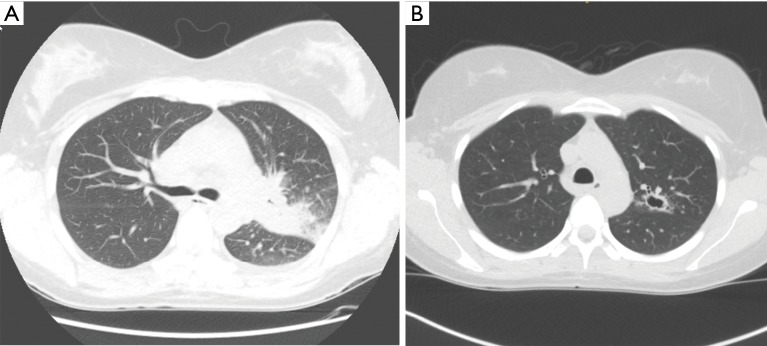
Pulmonary coccidioidomycosis. (A) Acute pulmonary coccidioidomycosis infection in a kidney transplant patient showing left upper lobe consolidation; (B) evolution of the left upper lobe consolidation into a central thick walled cavity despite antifungal therapy in the same post-transplant patient.
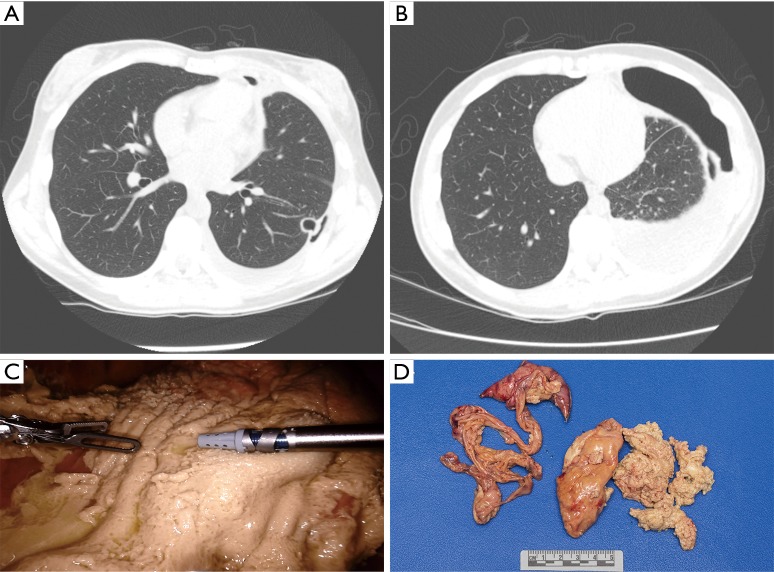
Coccidioidomycosis empyema. (A) Peripheral left lower lobe coccidioidomycosis cavity with evidence of perforation into the pleural space resulting in a small hydropneumothorax; (B) progression of the hydropneumothorax with pleural fluid cultures positive for coccidioidomycosis; (C) robotic decortication of the left coccidioidomycosis empyema. There is a significant pleural rind encompassing the entire left lung; (D) surgical specimen from the completed decortication. The uppermost specimen is the wedge resection of the left lower lobe where the perforated cavity was located. The remainder of the tissue is the visceral pleural rind which was removed from the lung to allow re-expansion.

Chronic destructive pulmonary coccidioidomycosis of the left lung. There is complete obliteration of the left pulmonary parenchyma with associated pleural changes. There is contraction of the left hemothorax resulting in mediastinal shift. This patient also had significant left hemidiaphragm elevation from the pulmonary retraction.
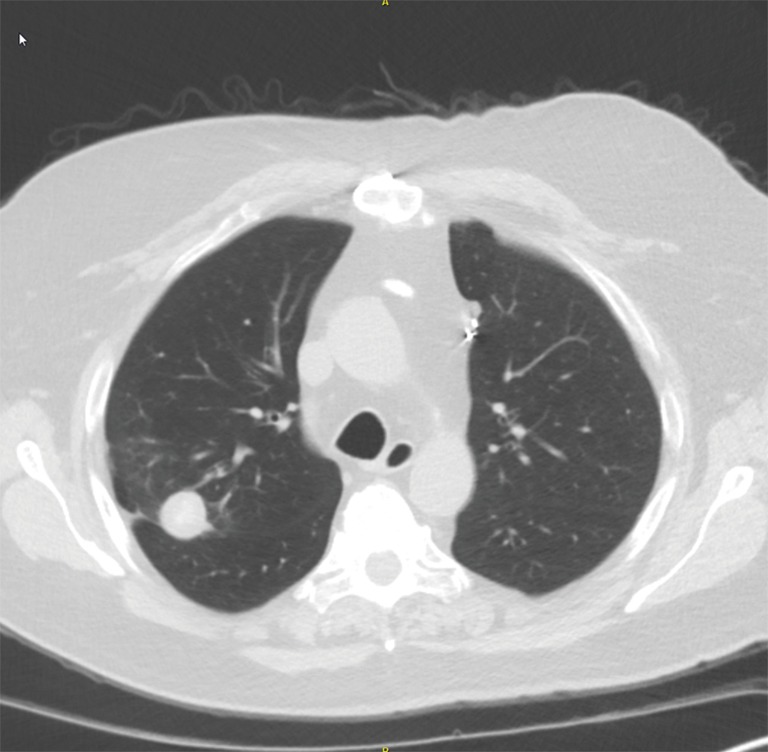
Pulmonary nodule caused by a prior histoplasmosis infection. The nodule enlarged over time and was avid on PET scan in a previous smoker with no history of fungal infection. Percutaneous biopsy was non-diagnostic. Surgical removal with a minimally invasive wedge resection was performed to rule out malignancy.
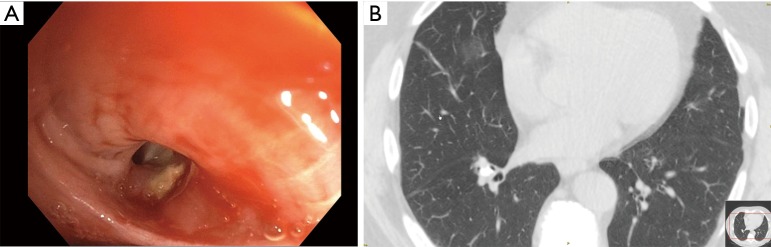
Broncholithiasis. (A) Bronchoscopy image in patient with broncholithiasis presenting with hemoptysis. A broncholith is seen in the right lower lobe segmental bronchus; (B) CT chest image corresponding with the broncholith visualized on bronchoscopy. The calcified area in the right lower lobe abuts both the right lower lobe airway and the associated pulmonary arteries.
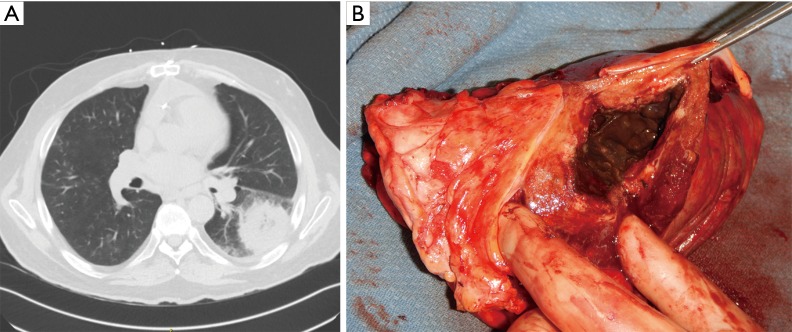
Pulmonary mucormycosis. (A) CT image of left lower lobe mucormycosis in a heart transplant recipient. The patient received a thoracotomy with left lower lobectomy and intercostal muscle flap to the bronchial stump; (B) surgical specimen (left lower lobectomy) with visualization of the mucormycosis cavity. There is extensive necrosis due to the angioinvasive nature of the fungus.
Similar articles
-
Common and emerging fungal pulmonary infections.Infect Dis Clin North Am. 2010 Sep;24(3):557-77. doi: 10.1016/j.idc.2010.04.003. Infect Dis Clin North Am. 2010. PMID: 20674792 Review.
-
Cavitary pulmonary infarct in immunocompromised hosts.Mayo Clin Proc. 1995 Jan;70(1):66-8. doi: 10.1016/S0025-6196(11)64668-5. Mayo Clin Proc. 1995. PMID: 7808055 Review.
-
Antifungal prophylaxis in lung transplantation.Semin Respir Crit Care Med. 2011 Dec;32(6):717-26. doi: 10.1055/s-0031-1295719. Epub 2011 Dec 13. Semin Respir Crit Care Med. 2011. PMID: 22167399 Review.
-
Pulmonary and sinus fungal diseases in non-immunocompromised patients.Lancet Infect Dis. 2017 Nov;17(11):e357-e366. doi: 10.1016/S1473-3099(17)30309-2. Epub 2017 Jul 31. Lancet Infect Dis. 2017. PMID: 28774699 Review.
-
The surgical management of fungal pulmonary infections in children with acute myelogenous leukemia.J Pediatr Surg. 1985 Dec;20(6):840-4. doi: 10.1016/s0022-3468(85)80052-x. J Pediatr Surg. 1985. PMID: 3866846
Cited by
-
The clinical and radiological characteristics of pulmonary cryptococcosis in immunocompetent and immunocompromised patients.BMC Pulm Med. 2021 Aug 13;21(1):262. doi: 10.1186/s12890-021-01630-3. BMC Pulm Med. 2021. PMID: 34389002 Free PMC article.
References
-
- Mitchell J. Infectious Lung Diseases. In: Selke F, del Nido P, Swanson S. editors. Sabiston and Spencer Surgery of the Chest. Philadelphia: Elsevier, 2016:205-26.
Publication types
LinkOut - more resources
Full Text Sources