

Management of broncholithiasis
- PMID: 30505529
- PMCID: PMC6218369
- DOI: 10.21037/jtd.2018.07.15
Management of broncholithiasis
Abstract
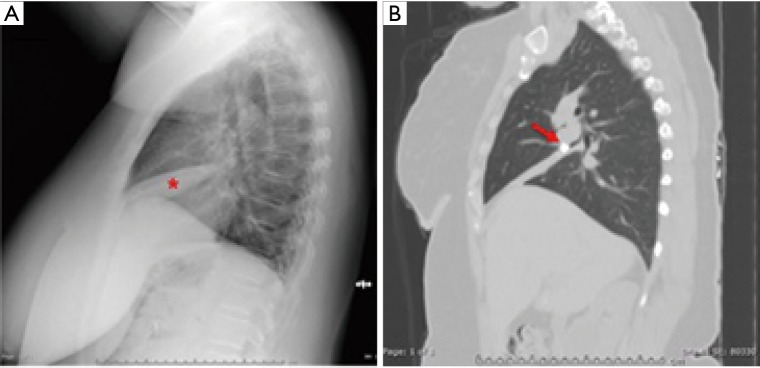
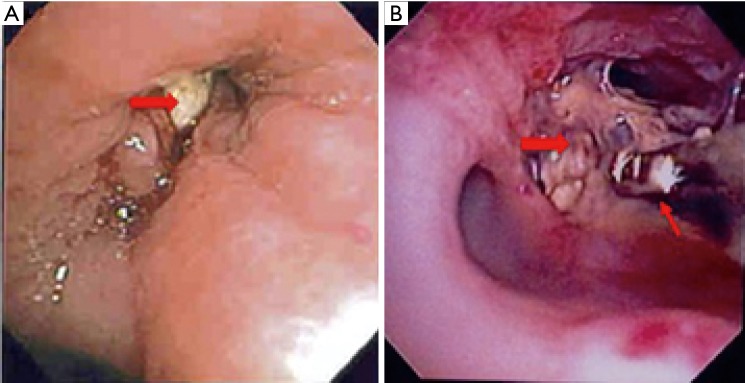
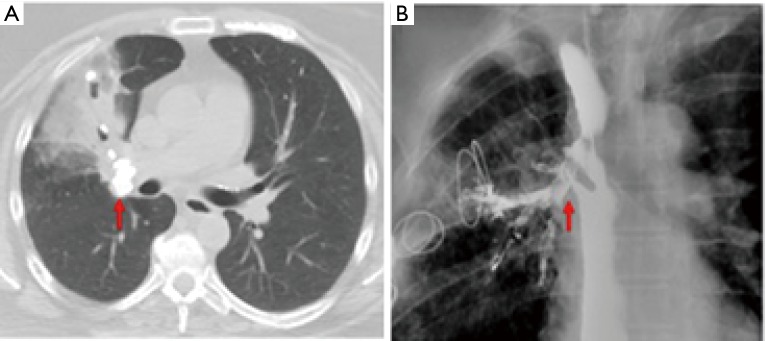
Broncholithiasis is a condition in which calcified material has entered the tracheobronchial tree, at times causing airway obstruction and inflammation. Broncholiths generally originate as calcified material in mediastinal lymph nodes that subsequently erode into adjacent airways, often as a result of prior granulomatous infection. Disease manifestations range from asymptomatic stones in the airway to life-threatening complications, including massive hemoptysis and post-obstructive pneumonia. Radiographic imaging, particularly computed tomography scanning of the chest, is integral in the evaluation of suspected broncholithiasis and can be helpful to assess involvement of adjacent structures, including vasculature, prior to any planned intervention. Management strategies largely depend on the severity of disease. Observation is warranted in asymptomatic cases, while therapeutic bronchoscopy and surgical interventions may be necessary for cases involving complications. Bronchoscopic extraction is often feasible in cases in which the broncholith is freely mobile within the airway, whereas partially-embedded broncholiths represent additional challenges. Surgical intervention is indicated for advanced cases deemed not amenable to endoscopic management. Complex cases involving complications such as massive hemoptysis and/or bronchomediastinal fistula formation are best managed with a multidisciplinary approach, utilizing expertise from fields such as pulmonology, radiology, and thoracic surgery.
Keywords: Surgical management; broncholithiasis; bronchoscopy.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

Similar articles
-
Broncholithiasis: A Review.Chest. 2019 Sep;156(3):445-455. doi: 10.1016/j.chest.2019.05.012. Epub 2019 Jun 4. Chest. 2019. PMID: 31173766 Review.
-
Broncholithiasis: Treatment Evaluation in 63 Patients.Am J Med Sci. 2022 Apr;363(4):351-358. doi: 10.1016/j.amjms.2021.05.028. Epub 2021 Aug 30. Am J Med Sci. 2022. PMID: 34473998
-
Broncholithiasis: a neglected bronchial disease in this country. Illustration of three cases.Changgeng Yi Xue Za Zhi. 1992 Mar;15(1):44-9. Changgeng Yi Xue Za Zhi. 1992. PMID: 1581838
-
Rigid bronchoscopy and surgical resection for broncholithiasis and calcified mediastinal lymph nodes.J Thorac Cardiovasc Surg. 2008 Jul;136(1):186-90. doi: 10.1016/j.jtcvs.2007.09.084. Epub 2008 May 19. J Thorac Cardiovasc Surg. 2008. PMID: 18603074
-
Broncholithiasis: review of the causes with radiologic-pathologic correlation.Radiographics. 2002 Oct;22 Spec No:S199-213. doi: 10.1148/radiographics.22.suppl_1.g02oc07s199. Radiographics. 2002. PMID: 12376611 Review.
Cited by
-
Case report of thoracoscopic resection for broncholithiasis with severe obstructive pneumonia.Indian J Thorac Cardiovasc Surg. 2020 Jan;36(1):74-77. doi: 10.1007/s12055-019-00870-7. Epub 2019 Oct 15. Indian J Thorac Cardiovasc Surg. 2020. PMID: 33061100 Free PMC article.
-
Combined Endoscopic Laser and Cryotherapy Management of Pediatric Central Airway Obstruction Secondary to a Histoplasmosis-Related Broncholith.Cureus. 2023 Sep 18;15(9):e45492. doi: 10.7759/cureus.45492. eCollection 2023 Sep. Cureus. 2023. PMID: 37859920 Free PMC article.
-
Successful removal of a broncholith using a cryo-probe under rigid bronchoscopy: A case report.Respirol Case Rep. 2022 Aug 19;10(9):e01024. doi: 10.1002/rcr2.1024. eCollection 2022 Sep. Respirol Case Rep. 2022. PMID: 36000084 Free PMC article.
-
A 75-year-old man with transbronchial broncholithiasis followed up for 9 years!J Postgrad Med. 2023 Apr-Jun;69(2):116-117. doi: 10.4103/jpgm.jpgm_156_22. J Postgrad Med. 2023. PMID: 36930547 Free PMC article. No abstract available.
-
Feasibility and long-term safety of Ho:YAG laser lithotripsy in broncholithiasis patients.BMC Pulm Med. 2021 Mar 10;21(1):81. doi: 10.1186/s12890-021-01407-8. BMC Pulm Med. 2021. PMID: 33691662 Free PMC article.
References
-
- Dixon GF, Donnerberg RL, Schonfeld SA, et al. Advances in the diagnosis and treatment of broncholithiasis. Am Rev Respir Dis 1984;129:1028-30. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Molecular Biology Databases