

doi: 10.21037/jtd.2018.06.147.
Massive hemoptysis in pulmonary infections: bronchial artery embolization
Affiliations
- PMID: 30505533
- PMCID: PMC6218368
- DOI: 10.21037/jtd.2018.06.147
Item in Clipboard
Massive hemoptysis in pulmonary infections: bronchial artery embolization
J Thorac Dis.
2018 Oct.
No abstract available
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures

A 37-year-old female from Peru with history of multiple episodes of hemoptysis. The patient has undergone treatment for tuberculosis both in Peru and in the United States after emigrating. (A) Coronally reconstructed CT image demonstrates a cavitary mass in the right upper lobe (arrow); (B) aortogram demonstrates a hypertrophied right ICBT (arrowhead) and hypervascularity in the region of the lesion (arrow); (C) repeat digital subtraction angiogram after selective catheterization of the right ICBT and superselective catheterization with a microcatheter redemonstrates the hypervascularity; (D) digital subtraction angiogram after embolization demonstrates no residual flow to the lesion.

A 63-year-old woman who presents with massive hemoptysis. She has a known history of Histoplasmosis for which a right lower lobe wedge resection was performed approximately 15 years ago. In the resection margin, the patient has developed a partially calcified cavitary lesion which has been slowly increasing in size. Bronchoscopic biopsies performed approximately one month earlier were negative for malignancy. (A) Coronally reconstructed CT image demonstrates a partially calcified cavitary mass in the right lower lobe (arrowhead). Calcified left hilar nodes are noted as well (arrow); (B) digital subtraction angiogram from a selectively catheterized right ICBT demonstrates a hypertrophied lower branch of the artery supplying a hypervascular lesion (arrows). Incidentally noted is a hypervascular nodule in the upper lobe that corresponds to another nodule in the right upper lobe seen on CT (not shown); (C) unsubtracted angiogram demonstrates that the lower branch of the right has been selectively catheterized using a microcatheter. Embolization of this branch of the bronchial artery was performed using 300–500 µm microspheres; (D) post embolization angiogram from the proximal right ICBT demonstrates no flow to the embolized branch or right lower lobe lesion. It was felt that the large right lower cavitary lesion was the likely culprit for the patient’s hemoptysis and hence the upper lobe branch was not embolized. Unfortunately, two days later the patient had repeat hemoptysis and was brought back down to the angiography suite; (E) pulmonary angiogram was performed which did not demonstrate any abnormalities; (F) selective catheterization of the upper branch of the right ICBT redemonstrates the hypervascular right upper lobe nodule. Embolization with 400 µm microspheres was performed (not shown). After this, the patient did not have repeat hemoptysis till her elective right lower lobectomy.
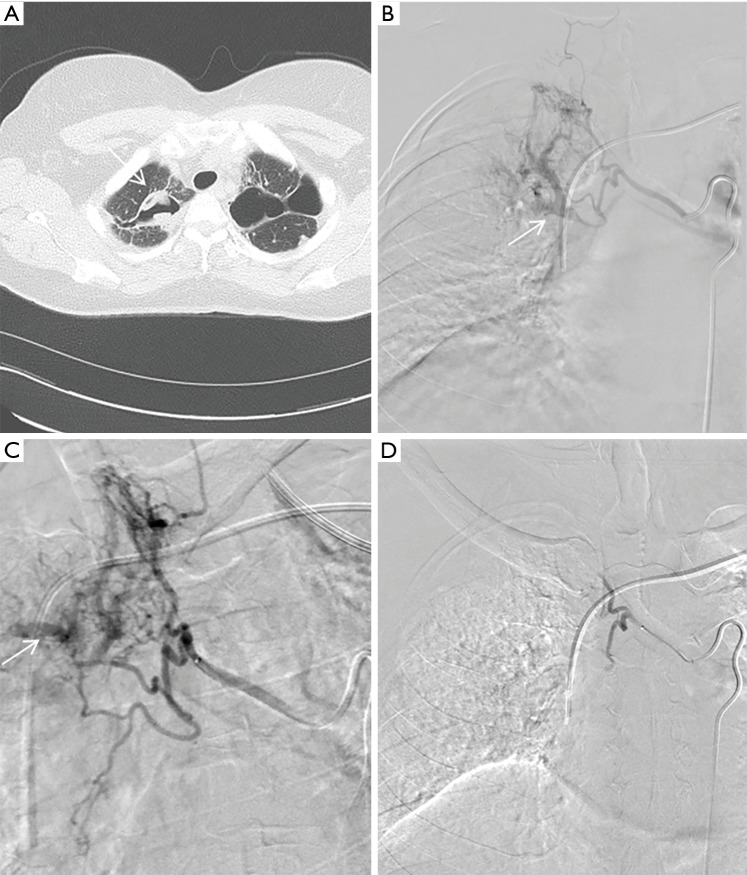
A 43-year-old female with history of pulmonary sarcoidosis complicated by a right upper lobe mycetoma with a history of recurrent hemoptysis treated by conservative measures as well as with intracavitary infusion of Amphotericin B. She now presents with multiple episodes of recurrent hemoptysis. Of note, bronchoalveolar lavage and sputum cultures in the past have been positive for Aspergillus fumigatus. (A) Axial CT image demonstrates a cavitary lesion in the right upper lobe with areas of soft tissue density which likely represents the aspergilloma; (B) digital subtraction angiogram after selective catheterization of the right ICBT demonstrates a hypervascular mass in the right upper lobe with filling of the pulmonary artery consistent with a shunt (arrow); (C) selective catheterization with a microcatheter redemonstrates the hypervascular mass and shunt (arrow); (D) digital subtraction angiogram after embolization with 700 µm microspheres demonstrates no residual flow to the lesion.
References
-
- Remy J, Voisin C, Ribet M, et al. Treatment, by embolization, of severe or repeated hemoptysis associated with systemic hypervascularization. Nouv Presse Med 1973;2:2060. - PubMed
LinkOut - more resources
Full Text Sources