

Endoscopic stenting should be advocated in patients with stage IV colorectal cancer presenting with acute obstruction
- PMID: 30505576
- PMCID: PMC6219967
- DOI: 10.21037/jgo.2018.06.03
Endoscopic stenting should be advocated in patients with stage IV colorectal cancer presenting with acute obstruction
Abstract
Background: It remains contentious whether endoscopic stenting or upfront surgery is more optimal in patients with metastatic colorectal cancers presenting with large bowel obstruction.
Methods: A retrospective review of all patients with metastatic colorectal cancer who underwent either endoscopic stenting or emergency surgery for acute large bowel obstruction was performed.
Results: Between January 2007 and June 2014, 66 patients, median age, 64 (range, 25-96) years, presented with acute large bowel obstruction from metastatic colorectal cancer. Forty (60.6%) patients underwent endoscopic stenting whilst the rest received immediate upfront surgical intervention. Of the 40 patients, 29 (72.5%) were successfully stented. The remaining 11 (27.5%) patients who failed endoscopic stenting required immediate emergency surgery to relieve the obstruction. Patients who failed endoscopic stenting had worse complications than those patients who had their stents successfully inserted [odds ratio (OR), 23.3; 95% confidence interval (CI), 2.29-250.00, P=0.004]. Patients who underwent emergency surgery had a longer median length of stay than patients who had successful endoscopic stenting (P=0.003). The patients that underwent successful stenting had earlier commencement of chemotherapy compared to those who had upfront surgery (P=0.02). There was no difference in stoma creation rates between patients who had emergency surgery versus those who were successfully stented.
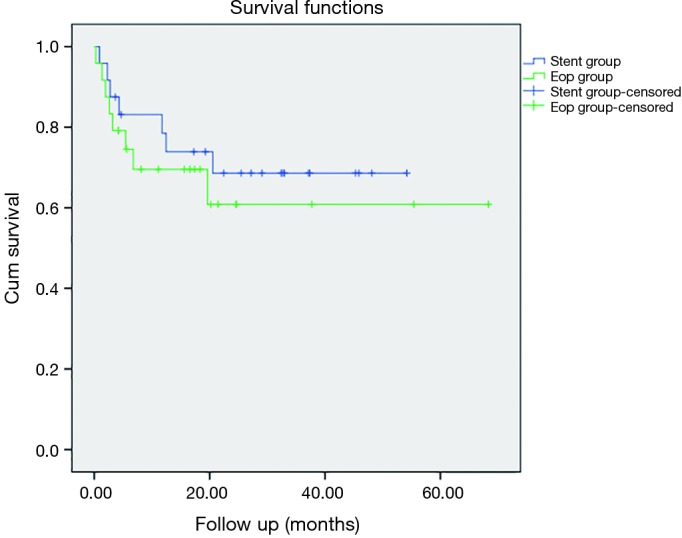
Conclusions: Stenting is a safe option in patients with stage IV colorectal cancer presenting with acute large bowel obstruction. Earlier commencement of chemotherapy occurs in patients who were successfully stented. Patients who failed stenting have equivalent outcomes to those who undergone upfront emergency surgery.
Keywords: Metastatic; colorectal cancer; stenting; treatment outcome.
Conflict of interest statement
Conflicts of Interest: The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Endoscopic Stenting Does Not Worsen Long Term Outcomes Amongst Patients Presenting with Obstruction from Colorectal Cancers.Ann Surg Oncol. 2017 Jun;24(6):1618-1625. doi: 10.1245/s10434-016-5724-z. Epub 2017 Jan 4. Ann Surg Oncol. 2017. PMID: 28054189
-
Patients who failed endoscopic stenting for left-sided malignant colorectal obstruction suffered the worst outcomes.Int J Colorectal Dis. 2014 Oct;29(10):1267-73. doi: 10.1007/s00384-014-1948-1. Epub 2014 Jul 2. Int J Colorectal Dis. 2014. PMID: 24986142
-
Colorectal stenting for palliation and as a bridge to surgery: A 5-year follow-up study.World J Gastroenterol. 2015 Aug 21;21(31):9373-9. doi: 10.3748/wjg.v21.i31.9373. World J Gastroenterol. 2015. PMID: 26309363 Free PMC article.
-
Endoscopic stenting in colorectal cancer.J Gastrointest Oncol. 2019 Dec;10(6):1171-1182. doi: 10.21037/jgo.2019.02.15. J Gastrointest Oncol. 2019. PMID: 31949937 Free PMC article. Review.
-
Comparison of colonic stenting and open surgery for malignant large bowel obstruction.Surg Endosc. 2007 Feb;21(2):225-33. doi: 10.1007/s00464-005-0644-1. Epub 2006 Dec 9. Surg Endosc. 2007. PMID: 17160651 Review.
Cited by
-
Comparison of colonic stents, stomas and resection for obstructive left colon cancer: a meta-analysis.Tech Coloproctol. 2020 Nov;24(11):1121-1136. doi: 10.1007/s10151-020-02296-5. Epub 2020 Jul 17. Tech Coloproctol. 2020. PMID: 32681344 Review.
-
Laparoscopic versus open surgery in obstructive colorectal cancer patients following stents placement: a comprehensive meta-analysis of cohort studies.Surg Endosc. 2024 Apr;38(4):1740-1757. doi: 10.1007/s00464-024-10710-4. Epub 2024 Mar 5. Surg Endosc. 2024. PMID: 38443501 Free PMC article.
-
Stage IV Colorectal Cancer at Initial Presentation versus Progression during and after Treatment, Differences in Management: Management Differences for Initial Presentation versus Progression of Disease after Initial Treatment.Clin Colon Rectal Surg. 2023 Apr 16;37(2):108-113. doi: 10.1055/s-0043-1761626. eCollection 2024 Mar. Clin Colon Rectal Surg. 2023. PMID: 38322603 Free PMC article. Review.
-
Controversies of colonic stenting in obstructive left colorectal cancer: a critical analysis with meta-analysis and meta-regression.Int J Colorectal Dis. 2021 Apr;36(4):689-700. doi: 10.1007/s00384-021-03834-9. Epub 2021 Jan 25. Int J Colorectal Dis. 2021. PMID: 33495871 Review.
-
Case report: Stent-first strategy as a potential approach in the management of malignant right-sided colonic obstruction with cardiovascular risks.Front Surg. 2022 Sep 22;9:1006020. doi: 10.3389/fsurg.2022.1006020. eCollection 2022. Front Surg. 2022. PMID: 36211276 Free PMC article.
References
LinkOut - more resources
Full Text Sources