

How I deploy arterial grafts
- PMID: 30505755
- PMCID: PMC6219946
- DOI: 10.21037/acs.2018.09.06
How I deploy arterial grafts
Abstract
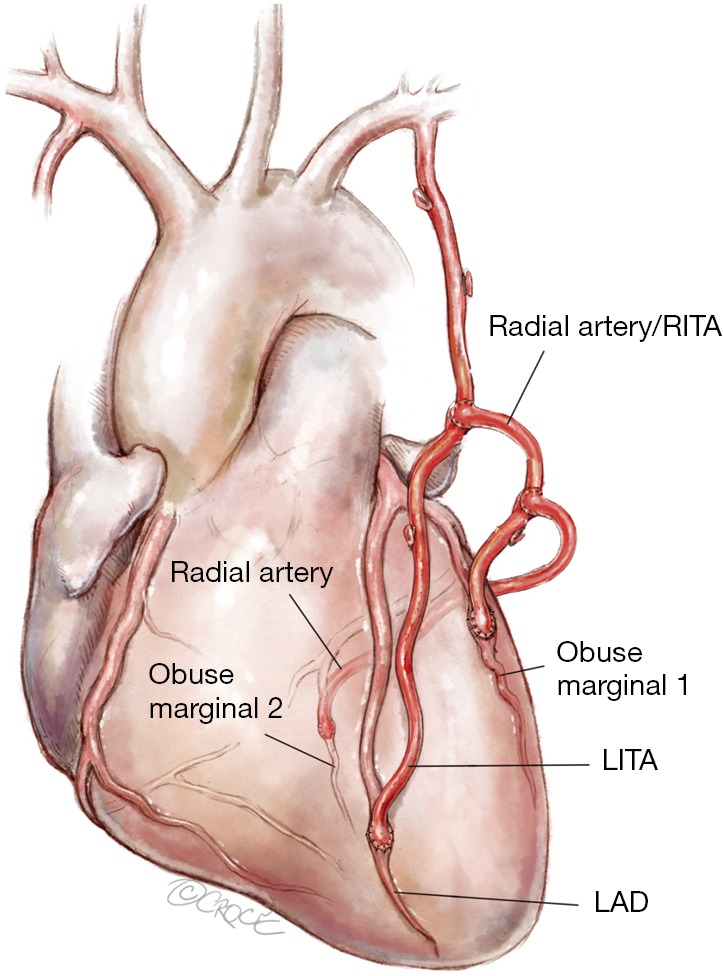
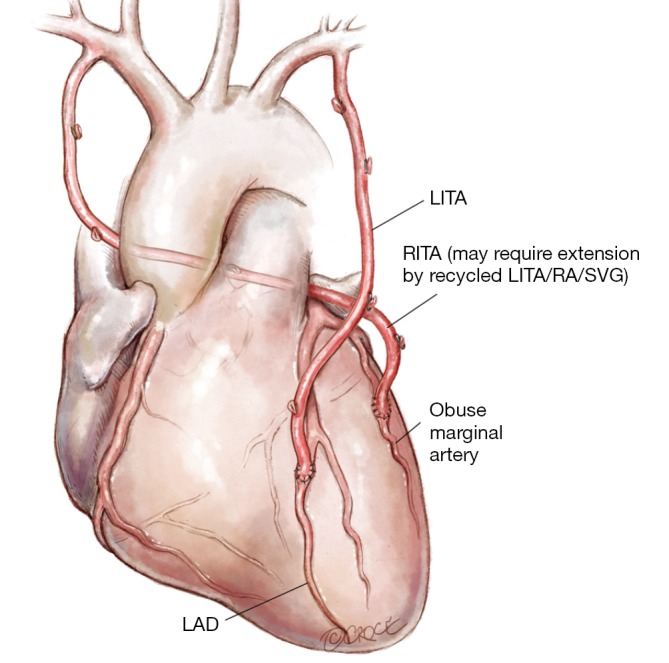
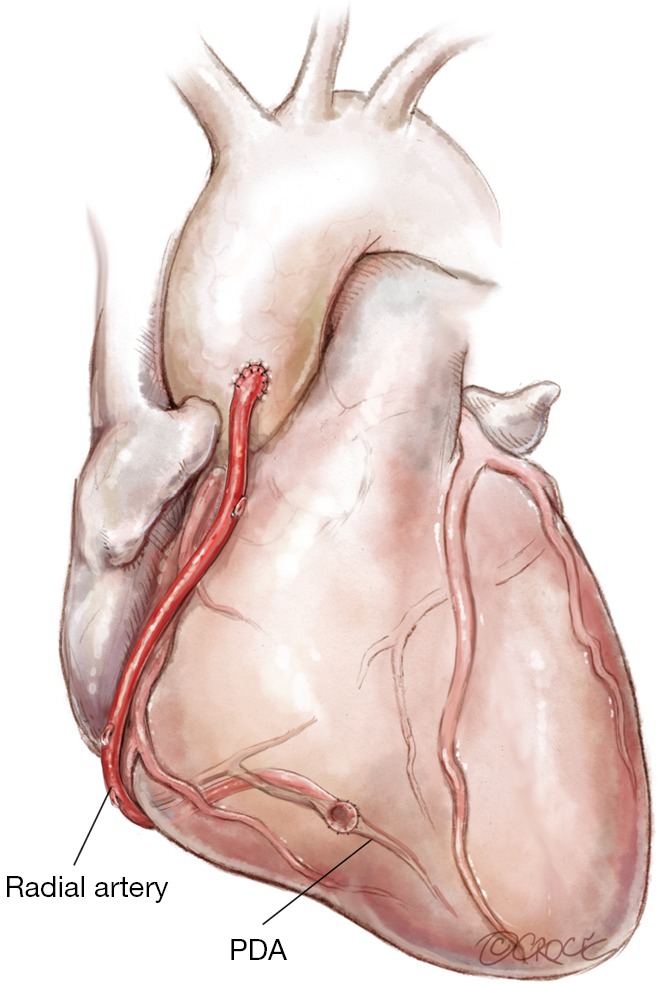
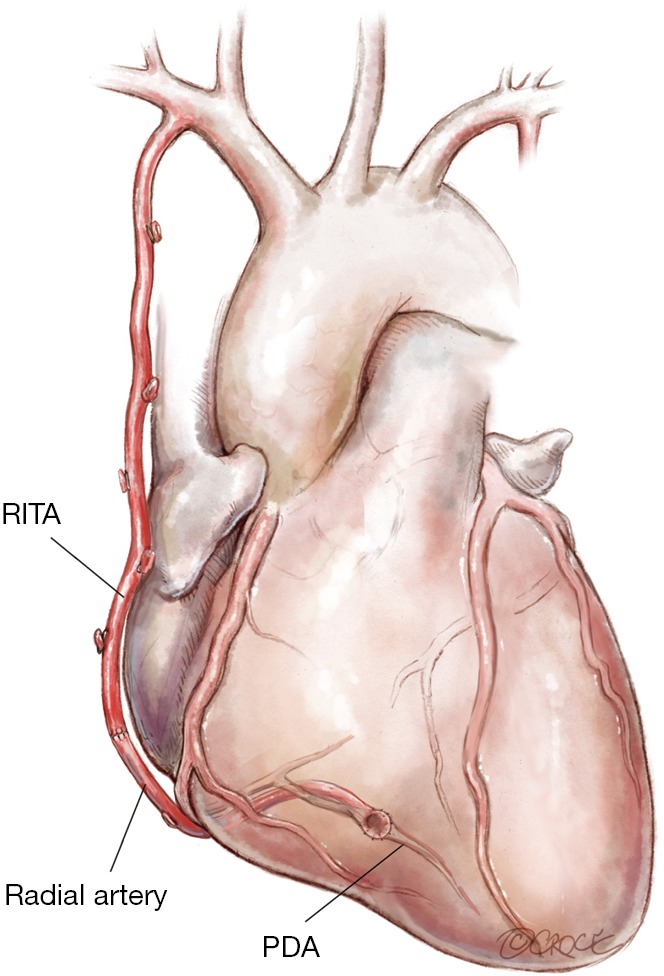
There are currently around one million coronary artery bypass graft (CABG) procedures performed worldwide annually and despite two decades of evidence to support the use of a second arterial graft, if not total arterial grafting, the stark reality is that in contemporary practice 80% of all grafts used for CABG are saphenous vein grafts (SVG). The following description of how I deploy arterial grafts has been developed over more than two decades of clinical practice and largely self-taught by a process of "trial and error" and most importantly dictated by "ease of use" rather than personal robust angiographic data of long-term patency (although there is other such existing data in the literature for some of these techniques). The fact that there are numerous potential variants of deploying multiple arterial grafts underpins the fact that there is no single operation that is ideal in every patient-it is not a case of "one size fits all" as would be the situation for the use of a single internal thoracic artery (ITA) and supplemental vein grafts.
Keywords: Internal thoracic artery (ITA); coronary artery bypass graft (CABG); off-pump; radial artery (RA).
Conflict of interest statement
Conflicts of Interest: Prof. DP Taggart has received research funding, speaking and travelling honoraria from Medistim (Oslo) and is the Principle Investigator for the REQUEST Registry (funded by Medistim).
Figures
References
Publication types
LinkOut - more resources
Full Text Sources