

Global, regional, and national burden of meningitis, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016
- PMID: 30507391
- PMCID: PMC6234314
- DOI: 10.1016/S1474-4422(18)30387-9
Global, regional, and national burden of meningitis, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016
Erratum in
-
Correction to Lancet Neurol 2018; 17: 1061-82.Lancet Neurol. 2021 Dec;20(12):e7. doi: 10.1016/S1474-4422(21)00381-1. Lancet Neurol. 2021. PMID: 34800418 Free PMC article. No abstract available.
Abstract
Background: Acute meningitis has a high case-fatality rate and survivors can have severe lifelong disability. We aimed to provide a comprehensive assessment of the levels and trends of global meningitis burden that could help to guide introduction, continuation, and ongoing development of vaccines and treatment programmes.
Methods: The Global Burden of Diseases, Injuries, and Risk Factors (GBD) 2016 study estimated meningitis burden due to one of four types of cause: pneumococcal, meningococcal, Haemophilus influenzae type b, and a residual category of other causes. Cause-specific mortality estimates were generated via cause of death ensemble modelling of vital registration and verbal autopsy data that were subject to standardised data processing algorithms. Deaths were multiplied by the GBD standard life expectancy at age of death to estimate years of life lost, the mortality component of disability-adjusted life-years (DALYs). A systematic analysis of relevant publications and hospital and claims data was used to estimate meningitis incidence via a Bayesian meta-regression tool. Meningitis deaths and cases were split between causes with meta-regressions of aetiological proportions of mortality and incidence, respectively. Probabilities of long-term impairment by cause of meningitis were applied to survivors and used to estimate years of life lived with disability (YLDs). We assessed the relationship between burden metrics and Socio-demographic Index (SDI), a composite measure of development based on fertility, income, and education.
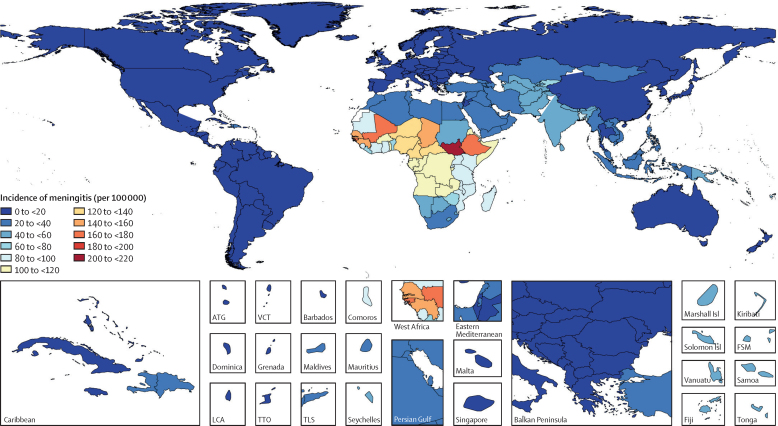
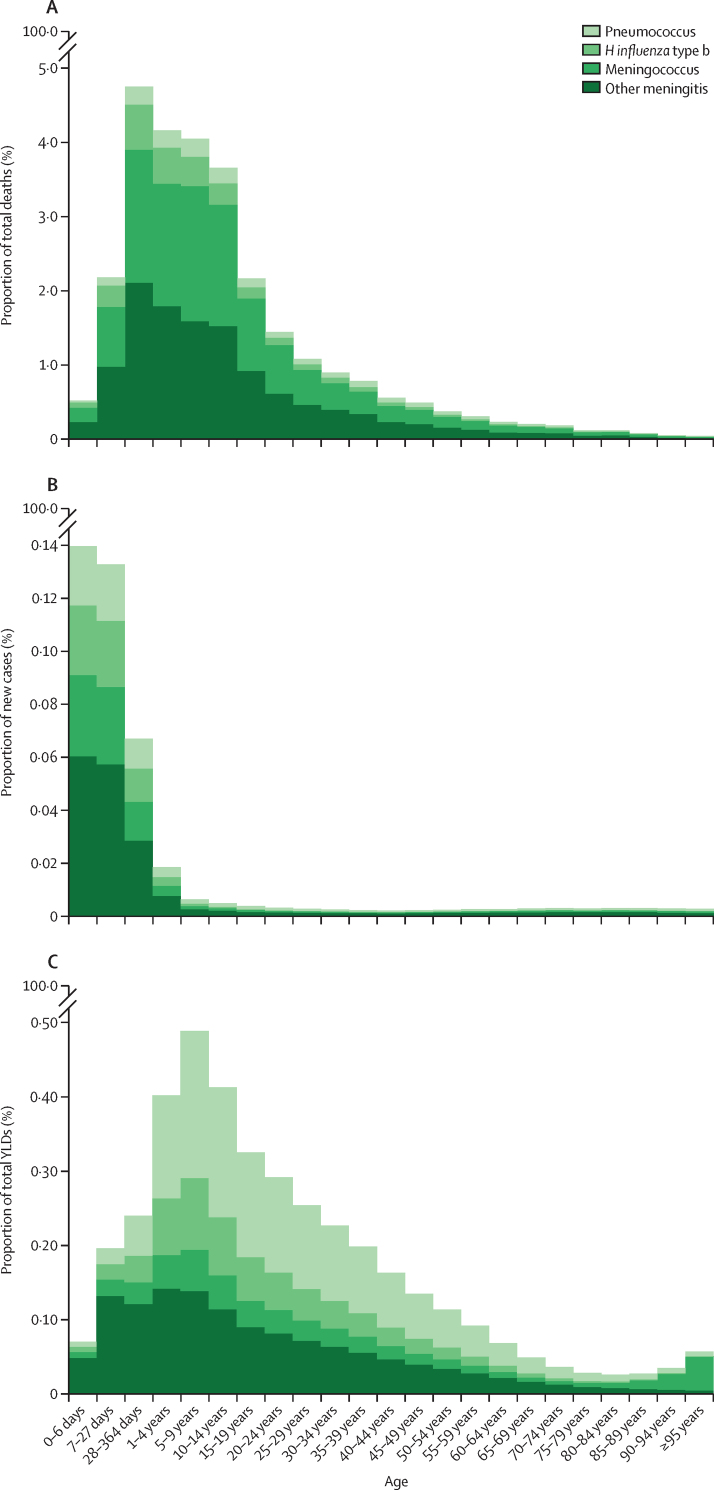
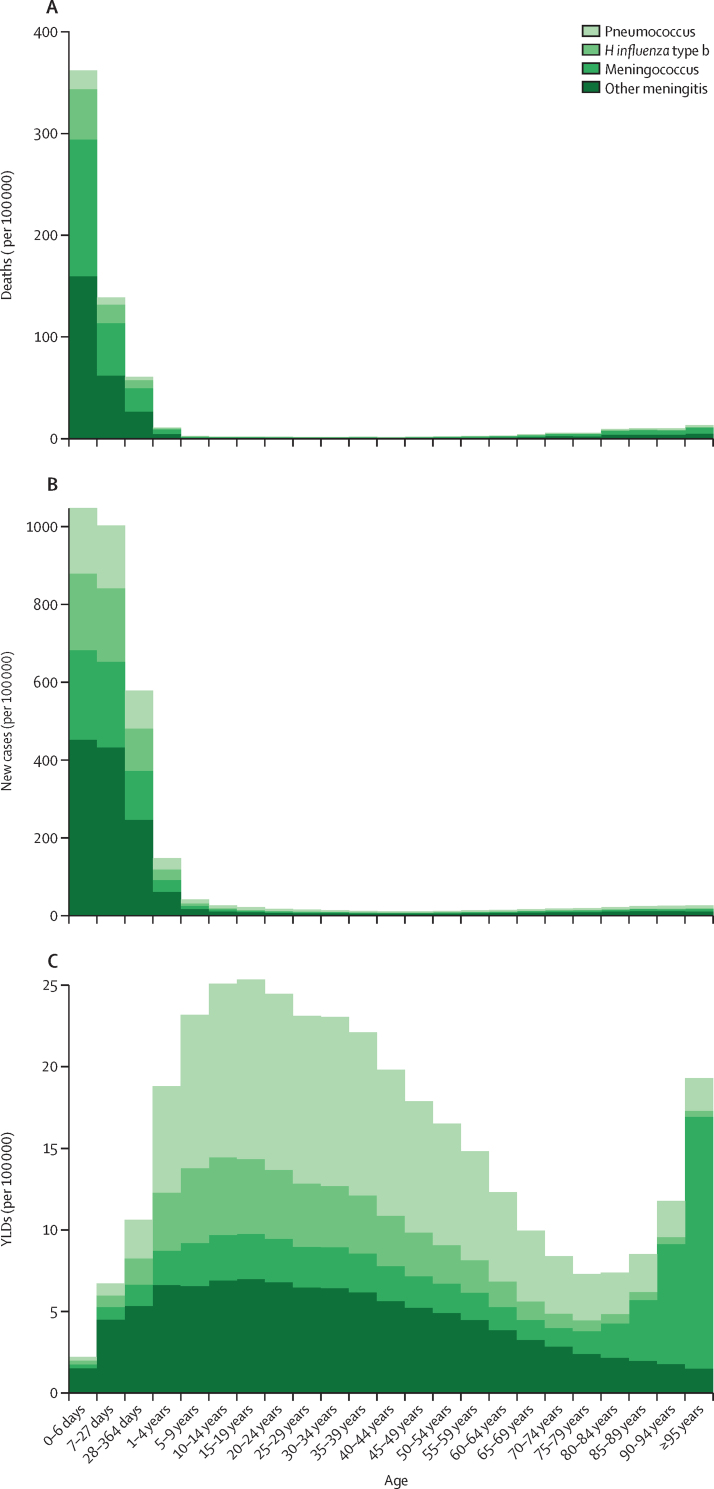
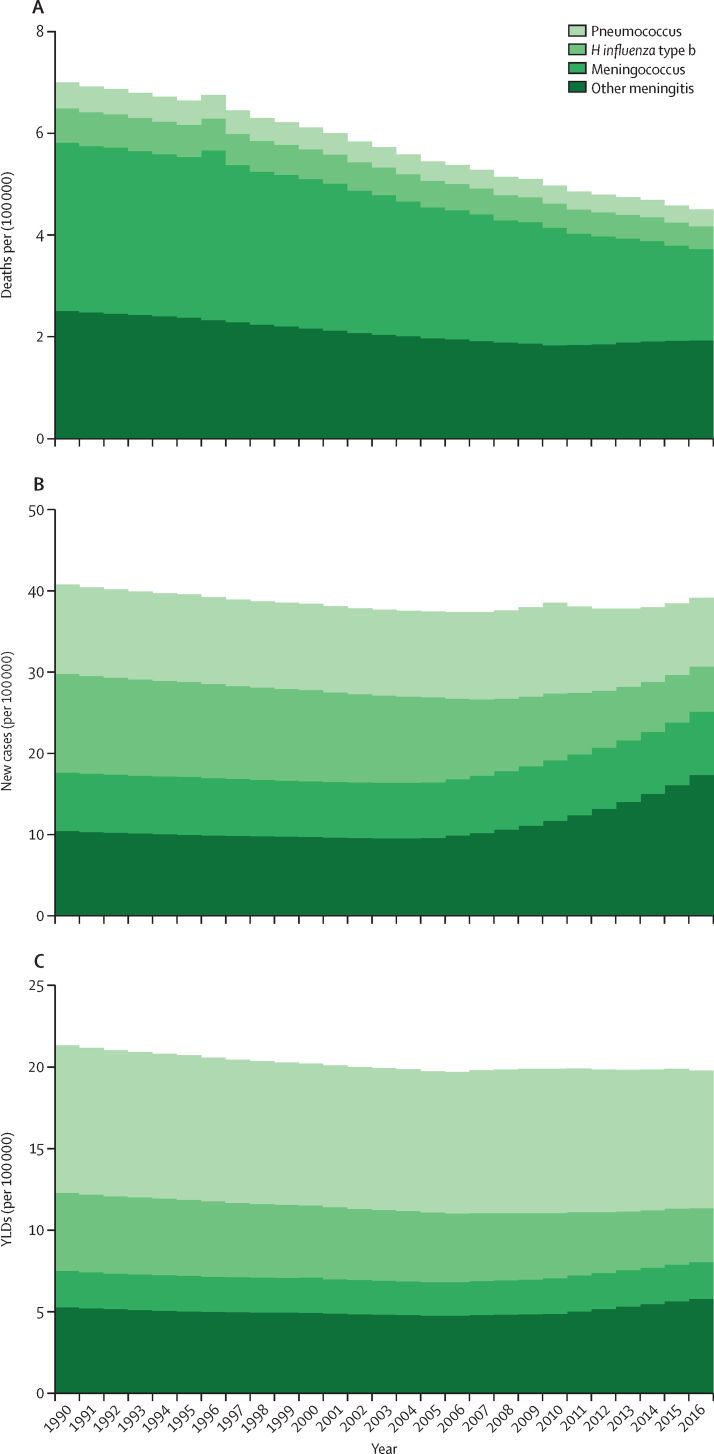
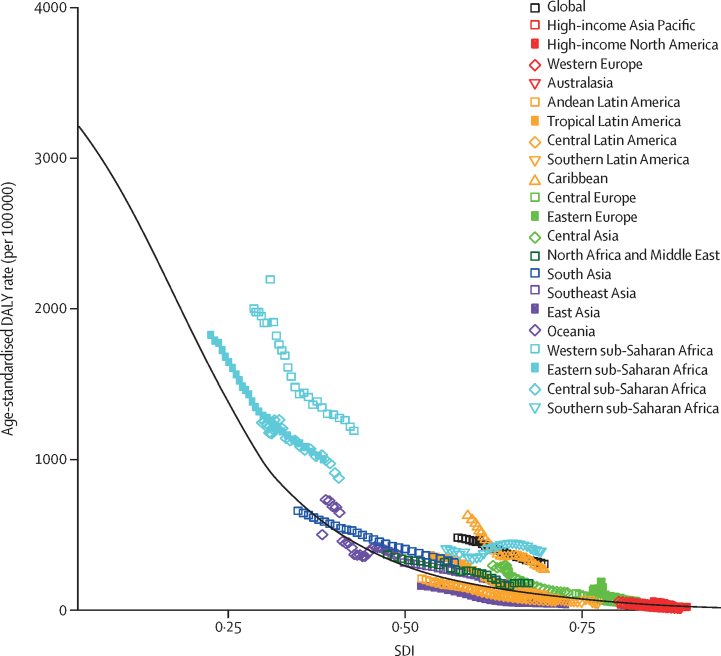
Findings: Global meningitis deaths decreased by 21·0% from 1990 to 2016, from 403 012 (95% uncertainty interval [UI] 319 426-458 514) to 318 400 (265 218-408 705). Incident cases globally increased from 2·50 million (95% UI 2·19-2·91) in 1990 to 2·82 million (2·46-3·31) in 2016. Meningitis mortality and incidence were closely related to SDI. The highest mortality rates and incidence rates were found in the peri-Sahelian countries that comprise the African meningitis belt, with six of the ten countries with the largest number of cases and deaths being located within this region. Haemophilus influenzae type b was the most common cause of incident meningitis in 1990, at 780 070 cases (95% UI 613 585-978 219) globally, but decreased the most (-49·1%) to become the least common cause in 2016, with 397 297 cases (291 076-533 662). Meningococcus was the leading cause of meningitis mortality in 1990 (192 833 deaths [95% UI 153 358-221 503] globally), whereas other meningitis was the leading cause for both deaths (136 423 [112 682-178 022]) and incident cases (1·25 million [1·06-1·49]) in 2016. Pneumococcus caused the largest number of YLDs (634 458 [444 787-839 749]) in 2016, owing to its more severe long-term effects on survivors. Globally in 2016, 1·48 million (1·04-1·96) YLDs were due to meningitis compared with 21·87 million (18·20-28·28) DALYs, indicating that the contribution of mortality to meningitis burden is far greater than the contribution of disabling outcomes.
Interpretation: Meningitis burden remains high and progress lags substantially behind that of other vaccine-preventable diseases. Particular attention should be given to developing vaccines with broader coverage against the causes of meningitis, making these vaccines affordable in the most affected countries, improving vaccine uptake, improving access to low-cost diagnostics and therapeutics, and improving support for disabled survivors. Substantial uncertainty remains around pathogenic causes and risk factors for meningitis. Ongoing, active cause-specific surveillance of meningitis is crucial to continue and to improve monitoring of meningitis burdens and trends throughout the world.
Funding: Bill & Melinda Gates Foundation.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Bacterial meningitis: more can be done.Lancet Neurol. 2018 Dec;17(12):1028-1030. doi: 10.1016/S1474-4422(18)30397-1. Epub 2018 Nov 13. Lancet Neurol. 2018. PMID: 30507382 No abstract available.
References
-
- Baker M, McNicholas A, Garrett N. Household crowding a major risk factor for epidemic meningococcal disease in Auckland children. Pediatr Infect Dis J. 2000;19:983–990. - PubMed
-
- Miller L, Arakaki L, Ramautar A. Elevated risk for invasive meningococcal disease among persons with HIV. Ann Intern Med. 2014;160:30–37. - PubMed
-
- Hodgson A, Smith T, Gagneux S. Risk factors for meningococcal meningitis in northern Ghana. Trans R Soc Trop Med Hyg. 2001;95:477–480. - PubMed
-
- Battersby AJ, Knox-Macaulay HHM, Carrol ED. Susceptibility to invasive bacterial infections in children with sickle cell disease. Pediatr Blood Cancer. 2010;55:401–406. - PubMed
