

The Role of Cognitive Reserve in Alzheimer's Disease and Aging: A Multi-Modal Imaging Review
- PMID: 30507572
- PMCID: PMC8972845
- DOI: 10.3233/JAD-180549
The Role of Cognitive Reserve in Alzheimer's Disease and Aging: A Multi-Modal Imaging Review
Abstract
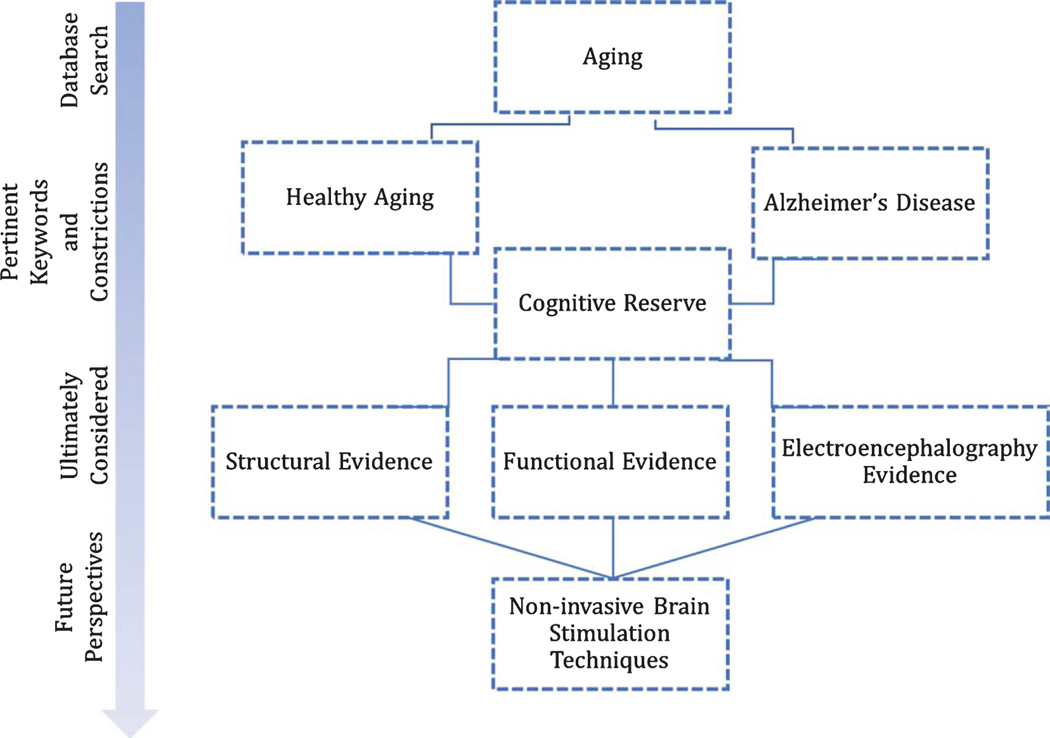
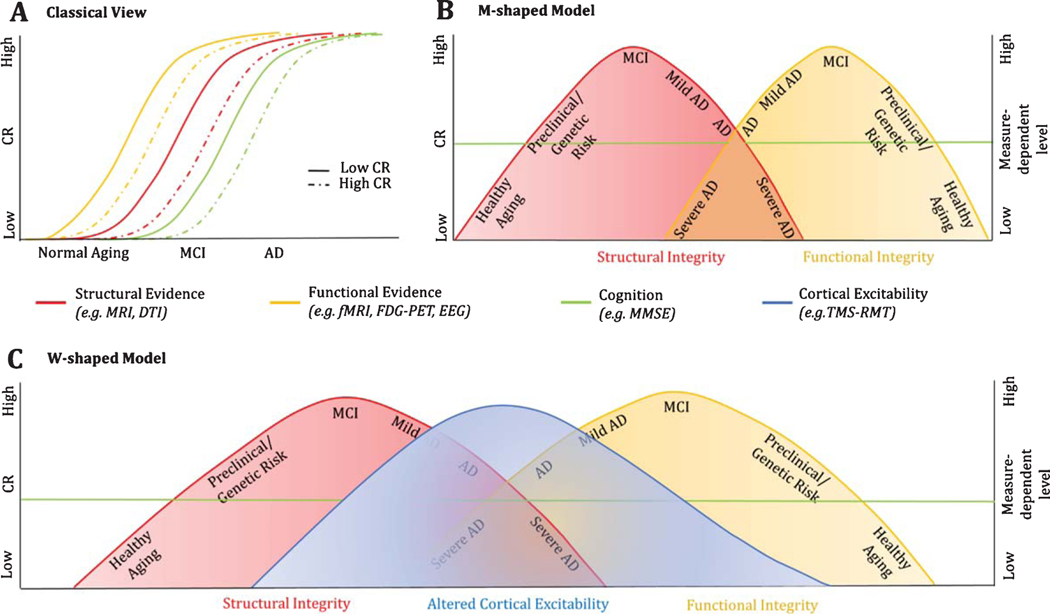
Comforts in modern society have generally been associated with longer survival rates, enabling individuals to reach advanced age as never before in history. With the increase in longevity, however, the incidence of neurodegenerative diseases, especially Alzheimer's disease, has also doubled. Nevertheless, most of the observed variance, in terms of time of clinical diagnosis and progression, often remains striking. Only recently, differences in the social, educational and occupational background of the individual, as proxies of cognitive reserve (CR), have been hypothesized to play a role in accounting for such discrepancies. CR is a well-established concept in literature; lots of studies have been conducted in trying to better understand its underlying neural substrates and associated biomarkers, resulting in an incredible amount of data being produced. Here, we aimed to summarize recent relevant published work addressing the issue, gathering evidence for the existence of a common path across research efforts that might ease future investigations by providing a general perspective on the actual state of the arts. An innovative model is hereby proposed, addressing the role of CR across structural and functional evidences, as well as the potential implementation of non-invasive brain stimulation techniques in the causal validation of such theoretical frame.
Keywords: Aging; Alzheimer’s disease; cognitive reserve; diffusion tensor imaging; electroencephalography; functional magnetic resonance imaging; magnetic resonance imaging; positron emission tomography; transcranial magnetic stimulation.
Figures
References
-
- Alzheimer’s Association (2017) 2017 Alzheimer’s disease facts and figures. Alzheimers Dement 13, 325–373.
-
- Driscoll I, Resnick SM, Troncoso JC, An Y, O’Brien R, Zonderman AB (2006) Impact of Alzheimer’s pathology on cognitive trajectories in nondemented elderly.AnnNeurol 60, 688–695. - PubMed
-
- Snowdon DA (2003) Healthy aging and dementia: Findings from the Nun Study. Ann Intern Med 139, 450–454. - PubMed
-
- Satz P (1993) Brain reserve capacity on symptom onset after brain injury: A formulation and review of evidence for threshold theory. Neuropsychology 7, 273–295.
-
- Katzman R (1993) Education and the prevalence of dementia and Alzheimer’s disease. Neurology 43, 13–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
