

Trends in Drug Use-Associated Infective Endocarditis and Heart Valve Surgery, 2007 to 2017: A Study of Statewide Discharge Data
- PMID: 30508432
- PMCID: PMC6548681
- DOI: 10.7326/M18-2124
Trends in Drug Use-Associated Infective Endocarditis and Heart Valve Surgery, 2007 to 2017: A Study of Statewide Discharge Data
Abstract
Background: Drug use-associated infective endocarditis (DUA-IE) is increasing as a result of the opioid epidemic. Infective endocarditis may require valve surgery, but surgical treatment of DUA-IE has invoked controversy, and the extent of its use is unknown.
Objective: To examine hospitalization trends for DUA-IE, the proportion of hospitalizations with surgery, patient characteristics, length of stay, and charges.
Design: 10-year analysis of a statewide hospital discharge database.
Setting: North Carolina hospitals, 2007 to 2017.
Patients: All patients aged 18 years or older hospitalized for IE.
Measurements: Annual trends in all IE admissions and in IE hospitalizations with valve surgery, stratified by patients' drug use status. Characteristics of DUA-IE surgical hospitalizations, including patient demographic characteristics, length of stay, disposition, and charges.
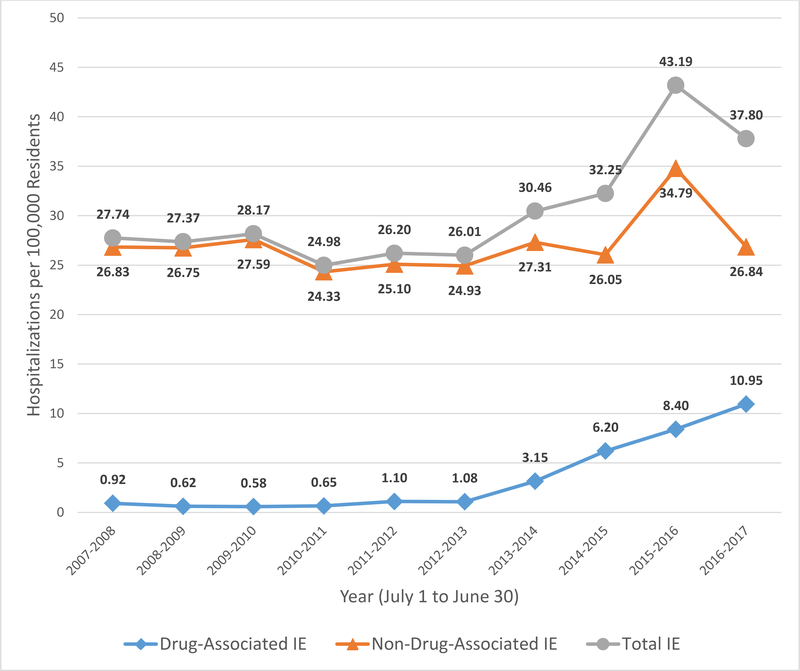
Results: Of 22 825 IE hospitalizations, 2602 (11%) were for DUA-IE. Valve surgery was performed in 1655 IE hospitalizations (7%), including 285 (17%) for DUA-IE. Annual DUA-IE hospitalizations increased from 0.92 to 10.95 and DUA-IE hospitalizations with surgery from 0.10 to 1.38 per 100 000 persons. In the final year, 42% of IE valve surgeries were performed in patients with DUA-IE. Compared with other surgical patients with IE, those with DUA-IE were younger (median age, 33 vs. 56 years), were more commonly female (47% vs. 33%) and white (89% vs. 63%), and were primarily insured by Medicaid (38%) or uninsured (35%). Hospital stays for DUA-IE were longer (median, 27 vs. 17 days), with higher median charges ($250 994 vs. $198 764). Charges for 282 DUA-IE hospitalizations exceeded $78 million.
Limitation: Reliance on administrative data and billing codes.
Conclusion: DUA-IE hospitalizations and valve surgeries increased more than 12-fold, and nearly half of all IE valve surgeries were performed in patients with DUA-IE. The swell of patients with DUA-IE is reshaping the scope, type, and financing of health care resources needed to effectively treat IE.
Primary funding source: National Institutes of Health.
Figures

Comment in
-
Drug-Associated Infective Endocarditis Trends: What's All the Buzz About?Ann Intern Med. 2019 Jan 1;170(1):68-69. doi: 10.7326/M18-3026. Epub 2018 Dec 4. Ann Intern Med. 2019. PMID: 30508422 Free PMC article. No abstract available.
References
-
- Wurcel AG, Anderson JE, Chui KKH, Skinner S, Knox TA, Snydman DR, et al. Increasing Infectious Endocarditis Admissions Among Young People Who Inject Drugs. Open Forum Infect Dis [Internet]. 2016. July 26 [cited 2017 Feb 27];3(3). Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC5084714/ - PMC - PubMed
-
- Rudd RA. Increases in Drug and Opioid-Involved Overdose Deaths — United States, 2010–2015. MMWR Morb Mortal Wkly Rep [Internet]. 2016. [cited 2017 May 12];65 Available from: http://www.cdc.gov/mmwr/volumes/65/wr/mm655051e1.htm - PubMed
-
- Deo SV, Raza S, Kalra A, Deo VS, Altarabsheh SE, Zia A, et al. Admissions for Infective Endocarditis in Intravenous Drug Users. J Am Coll Cardiol. 2018. April 10;71(14):1596–7. - PubMed
MeSH terms
Grants and funding
- R25 DA013582/DA/NIDA NIH HHS/United States
- R25 HL135304/HL/NHLBI NIH HHS/United States
- L30 AI140348/AI/NIAID NIH HHS/United States
- R34 AI122958/AI/NIAID NIH HHS/United States
- R25 HD076475/HD/NICHD NIH HHS/United States
- K12 HL138030/HL/NHLBI NIH HHS/United States
- KL2 TR001115/TR/NCATS NIH HHS/United States
- R01 DE023375/DE/NIDCR NIH HHS/United States
- UL1 TR001117/TR/NCATS NIH HHS/United States
- T32 AI070114/AI/NIAID NIH HHS/United States
- UG1 DA040317/DA/NIDA NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- R01 MD007658/MD/NIMHD NIH HHS/United States