

Assessment of small hepatocellular carcinoma: perfusion quantification and time-concentration curve evaluation using color-coded and quantitative digital subtraction angiography
- PMID: 30508937
- PMCID: PMC6283217
- DOI: 10.1097/MD.0000000000013392
Assessment of small hepatocellular carcinoma: perfusion quantification and time-concentration curve evaluation using color-coded and quantitative digital subtraction angiography
Abstract
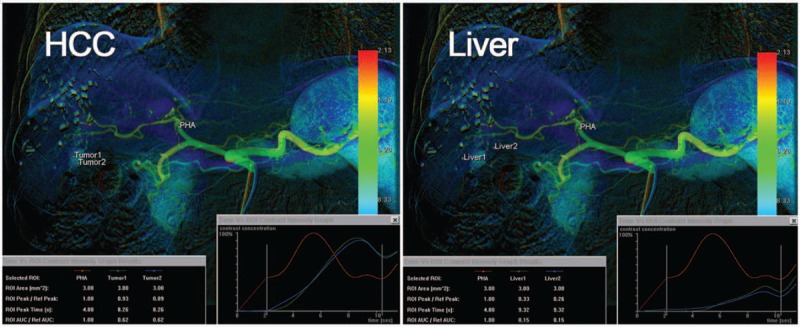
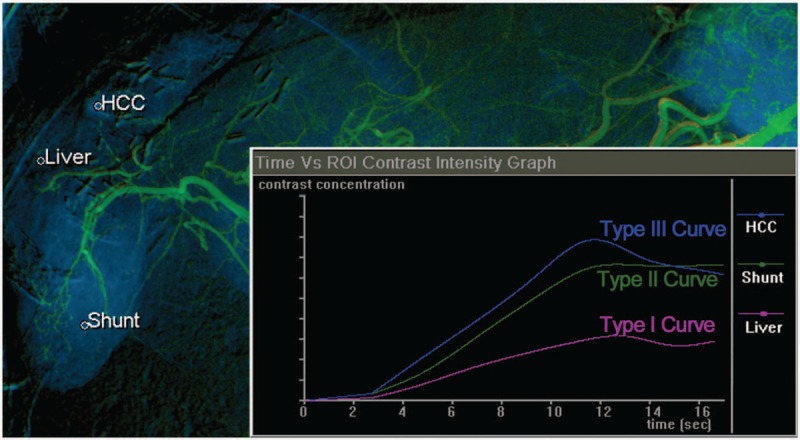
To explore the role of quantitative digital subtraction angiography (QDSA) in the diagnosis of small hepatocellular carcinoma (HCC).Between November 2015 and November 2017, all patients who underwent chemoembolization for HCC were retrospectively reviewed. Patients with tumors measuring more than 5 cm or evident post-processing imaging artifacts were excluded. Images were post-processed using the QDSA technique. Regions of interest were manually drawn on proper hepatic artery (as a reference), target HCC and peritumoral liver. Time-concentration curves and flow parameters of the peak ratio, subtracted time-to-peak (TTP), and area under the curve (AUC) ratio was obtained and analyzed.A total of 146 HCCs (mean diameter, 1.6 cm) of 71 cirrhotic patients (54 men, 17 women; mean age, 67.7 years) were enrolled. Compared with liver parenchyma, HCCs showed an increased and more rapid flow (peak ratio, AUC ratio, subtracted TTP, and wash-in slope; all P <.001). Compared with untreated HCCs, chemoembolized HCCs showed a slower flow (subtracted TTP and wash-in slope, P = .004 and .002, respectively). HCCs with a typical enhancement pattern on computed tomography (CT) or magnetic resonance imaging (MRI) had a trend toward Type III (washout pattern) time-concentration curves (P <.001). Chemoembolized HCCs had a trend toward Type II (plateau pattern) time-concentration curves (P = .005).QDSA technology can be used to quantify perfusion measurements of HCC and hepatic parenchyma and to assess perfusion changes after HCC chemoembolization.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Zaman SN, Johnson PJ, Williams R. Silent cirrhosis in patients with hepatocellular carcinoma. Implications for screening in high-incidence and low-incidence areas. Cancer 1990;65:1607–10. - PubMed
-
- Matsui O, Kadoya M, Yoshikawa J, et al. Small hepatocellular carcinoma: treatment with subsegmental transcatheter arterial embolization. Radiology 1993;188:79–83. - PubMed
-
- Itsubo M, Koike K, Tsuno S, et al. Subsegmental transcatheter arterial embolization for small hepatocellular carcinoma. Hepatogastroenterology 2002;49:735–9. - PubMed
-
- Sahani DV, Holalkere NS, Mueller PR, et al. Advanced hepatocellular carcinoma: CT perfusion of liver and tumor tissue—initial experience. Radiology 2007;243:736–43. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
