

Comparative Activity of Ceftriaxone, Ciprofloxacin, and Gentamicin as a Function of Bacterial Growth Rate Probed by Escherichia coli Chromosome Replication in the Mouse Peritonitis Model
- PMID: 30509946
- PMCID: PMC6355585
- DOI: 10.1128/AAC.02133-18
Comparative Activity of Ceftriaxone, Ciprofloxacin, and Gentamicin as a Function of Bacterial Growth Rate Probed by Escherichia coli Chromosome Replication in the Mouse Peritonitis Model
Abstract
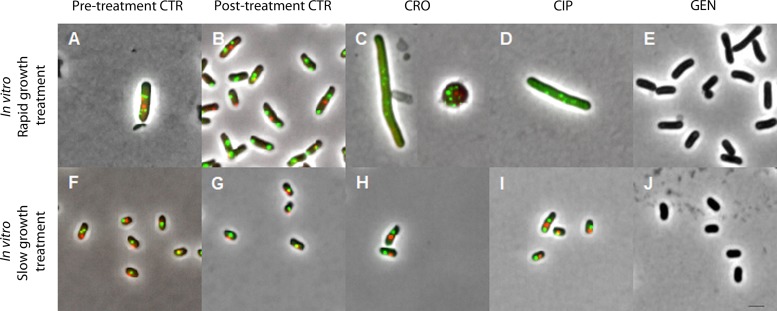
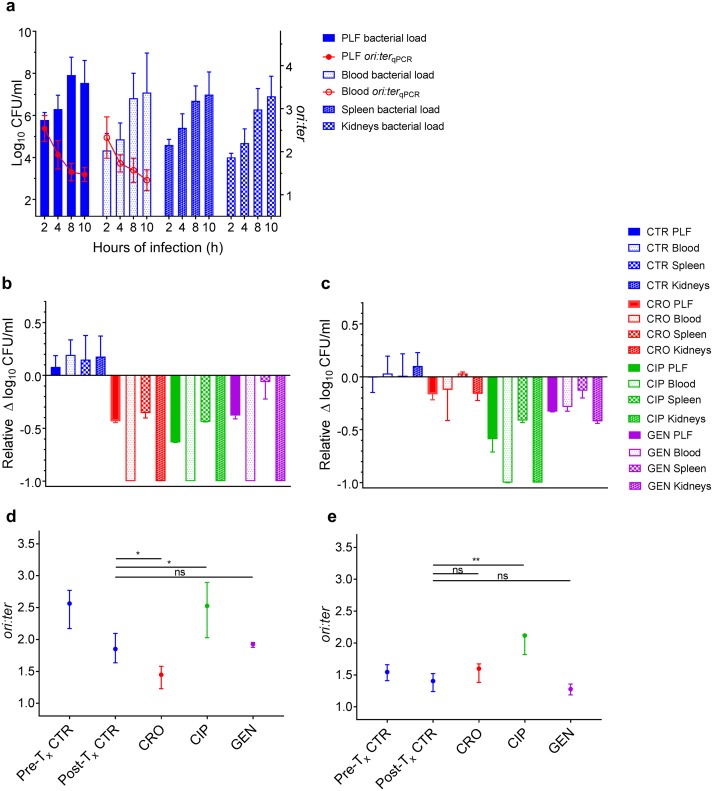
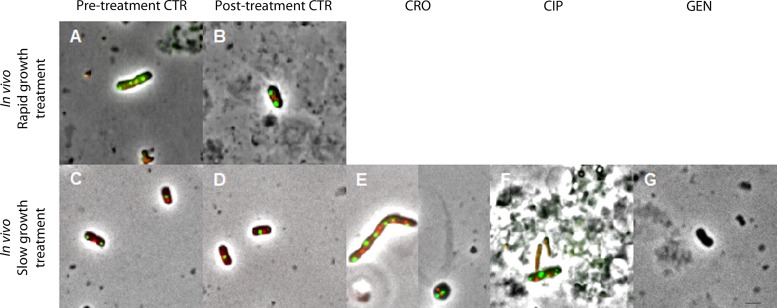
Commonly used antibiotics exert their effects predominantly on rapidly growing bacterial cells; yet, the growth dynamics taking place during infection in a complex host environment remain largely unknown. Hence, a means to measure in situ bacterial growth rate is essential to predict the outcome of antibacterial treatment. We have recently validated chromosome replication as a readout of in situ bacterial growth rate during Escherichia coli infection in the mouse peritonitis model. By the use of two complementary methods (quantitative PCR and fluorescence microscopy) for differential genome origin and terminus copy number quantification, we demonstrated the ability to track bacterial growth rate, both on a population average level and on a single-cell level, from one single biological specimen. Here, we asked whether the in situ growth rate predicts antibiotic treatment effect during infection in the same model. Parallel in vitro growth experiments were conducted as a proof of concept. Our data demonstrate that the activities of the commonly used antibiotics ceftriaxone and gentamicin correlated with pretreatment bacterial growth rate; both drugs performed better during rapid growth than during slow growth. Conversely, ciprofloxacin was less sensitive to bacterial growth rate, both in a homogenous in vitro bacterial population and in a more heterogeneous in vivo bacterial population. The method serves as a platform to test any antibiotic's dependency on active in situ bacterial growth. Improved insight into this relationship in vivo could ultimately prove helpful in evaluating future antibacterial strategies.
Keywords: Escherichia coli; bacterial growth; chromosome replication; experimental animal model.
Copyright © 2019 American Society for Microbiology.
Figures

References
-
- Kopf SH, Sessions AL, Cowley ES, Reyes C, Van Sambeek L, Hu Y, Orphan VJ, Kato R, Newman DK. 2016. Trace incorporation of heavy water reveals slow and heterogeneous pathogen growth rates in cystic fibrosis sputum. Proc Natl Acad Sci U S A 113:E110–E116. doi:10.1073/pnas.1512057112. - DOI - PMC - PubMed
-
- Olm MR, Brown CT, Brooks B, Firek B, Baker R, Burstein D, Soenjoyo K, Thomas BC, Morowitz M, Banfield JF. 2017. Identical bacterial populations colonize premature infant gut, skin, and oral microbiomes and exhibit different in situ growth rates. Genome Res 27:601–612. doi:10.1101/gr.213256.116. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
