

Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study
- PMID: 30510080
- PMCID: PMC6367644
- DOI: 10.1182/blood-2018-09-876136
Ravulizumab (ALXN1210) vs eculizumab in adult patients with PNH naive to complement inhibitors: the 301 study
Abstract
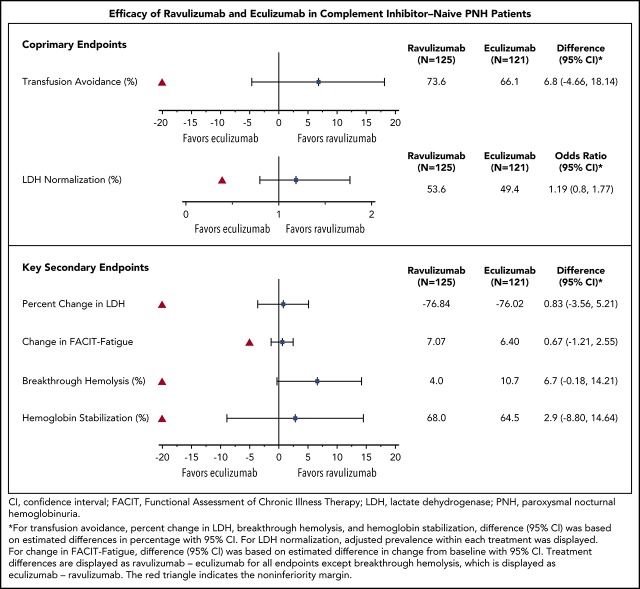
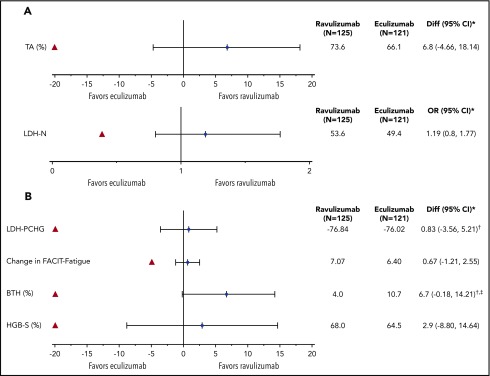
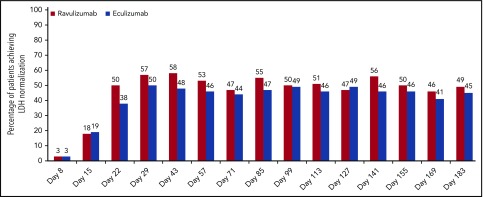
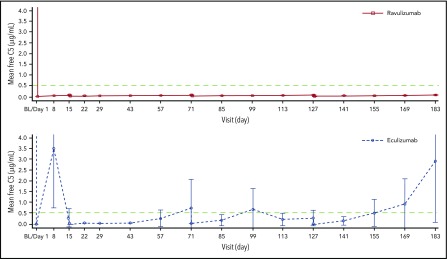
Ravulizumab (ALXN1210), a new complement C5 inhibitor, provides immediate, complete, and sustained C5 inhibition. This phase 3, open-label study assessed the noninferiority of ravulizumab to eculizumab in complement inhibitor-naive adults with paroxysmal nocturnal hemoglobinuria (PNH). Patients with lactate dehydrogenase (LDH) ≥1.5 times the upper limit of normal and at least 1 PNH symptom were randomized 1:1 to receive ravulizumab or eculizumab for 183 days (N = 246). Coprimary efficacy end points were proportion of patients remaining transfusion-free and LDH normalization. Secondary end points were percent change from baseline in LDH, change from baseline in Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue score, proportion of patients with breakthrough hemolysis, stabilized hemoglobin, and change in serum free C5. Ravulizumab was noninferior to eculizumab for both coprimary and all key secondary end points (Pinf < .0001): transfusion avoidance (73.6% vs 66.1%; difference of 6.8% [95% confidence interval (CI), -4.66, 18.14]), LDH normalization (53.6% vs 49.4%; odds ratio, 1.19 [0.80, 1.77]), percent reduction in LDH (-76.8% vs -76.0%; difference [95% CI], -0.83% [-5.21, 3.56]), change in FACIT-Fatigue score (7.07 vs 6.40; difference [95% CI], 0.67 [-1.21, 2.55]), breakthrough hemolysis (4.0% vs 10.7%; difference [95% CI], -6.7% [-14.21, 0.18]), and stabilized hemoglobin (68.0% vs 64.5%; difference [95% CI], 2.9 [-8.80, 14.64]). The safety and tolerability of ravulizumab and eculizumab were similar; no meningococcal infections occurred. In conclusion, ravulizumab given every 8 weeks achieved noninferiority compared with eculizumab given every 2 weeks for all efficacy end points, with a similar safety profile. This trial was registered at www.clinicaltrials.gov as #NCT02946463.
© 2019 by The American Society of Hematology.
Conflict of interest statement
Conflict-of-interest disclosure: J.W.L. has received honoraria, consulting fees, and research support (to Seoul St. Mary’s Hospital) from Alexion Pharmaceuticals, Inc. F.S.d.F. has received honoraria and research support (to St. Louis Hospital) from Alexion Pharmaceuticals, Inc. V. Pessoa and S.G. have received research support from Alexion Pharmaceuticals, Inc. W.F. has received honoraria from Alexion Pharmaceuticals, Inc, and Novartis. V. Ptushkin has received honoraria from Alexion Pharmaceuticals, Inc. S.T.R., L.V., L.S., R.A., and R.P. are employees and stockholders of Alexion Pharmaceuticals, Inc. H.S. has received honoraria and research support (all to University of Ulm) from Alexion Pharmaceuticals, Inc. A.H. has received honoraria and consulting fees from Alexion Pharmaceuticals, Inc. L.W.L.L. declares no competing financial interests.
Figures
Comment in
-
Ravulizumab: a complementary option for PNH.Blood. 2019 Feb 7;133(6):503-504. doi: 10.1182/blood-2018-12-891499. Blood. 2019. PMID: 30733201 No abstract available.
References
-
- Hillmen P, Young NS, Schubert J, et al. The complement inhibitor eculizumab in paroxysmal nocturnal hemoglobinuria. N Engl J Med. 2006;355(12):1233-1243. - PubMed
-
- Brodsky RA, Young NS, Antonioli E, et al. Multicenter phase 3 study of the complement inhibitor eculizumab for the treatment of patients with paroxysmal nocturnal hemoglobinuria. Blood. 2008;111(4):1840-1847. - PubMed
-
- Hillmen P, Muus P, Dührsen U, et al. Effect of the complement inhibitor eculizumab on thromboembolism in patients with paroxysmal nocturnal hemoglobinuria. Blood. 2007;110(12):4123-4128. - PubMed
-
- US Food and Drug Administration. Soliris (eculizumab); prescribing information. Boston, MA: Alexion Pharmaceuticals, Inc; 2018.
-
- European Medicines Agency. Soliris (eculizumab); summary of product characteristics. Paris, France: Alexion Europe SAS; 2017.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
