

Myelodysplastic syndrome progression to acute myeloid leukemia at the stem cell level
- PMID: 30510255
- PMCID: PMC6436966
- DOI: 10.1038/s41591-018-0267-4
Myelodysplastic syndrome progression to acute myeloid leukemia at the stem cell level
Erratum in
-
Publisher Correction: Myelodysplastic syndrome progression to acute myeloid leukemia at the stem cell level.Nat Med. 2019 Mar;25(3):529. doi: 10.1038/s41591-018-0333-y. Nat Med. 2019. PMID: 30568307
Abstract
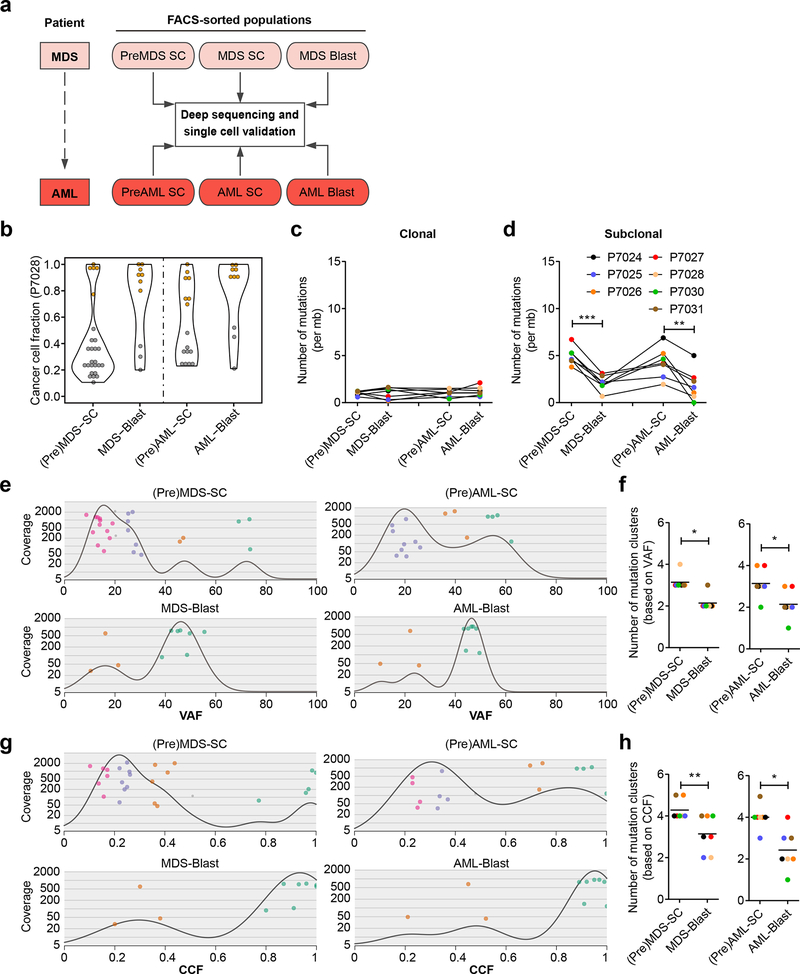
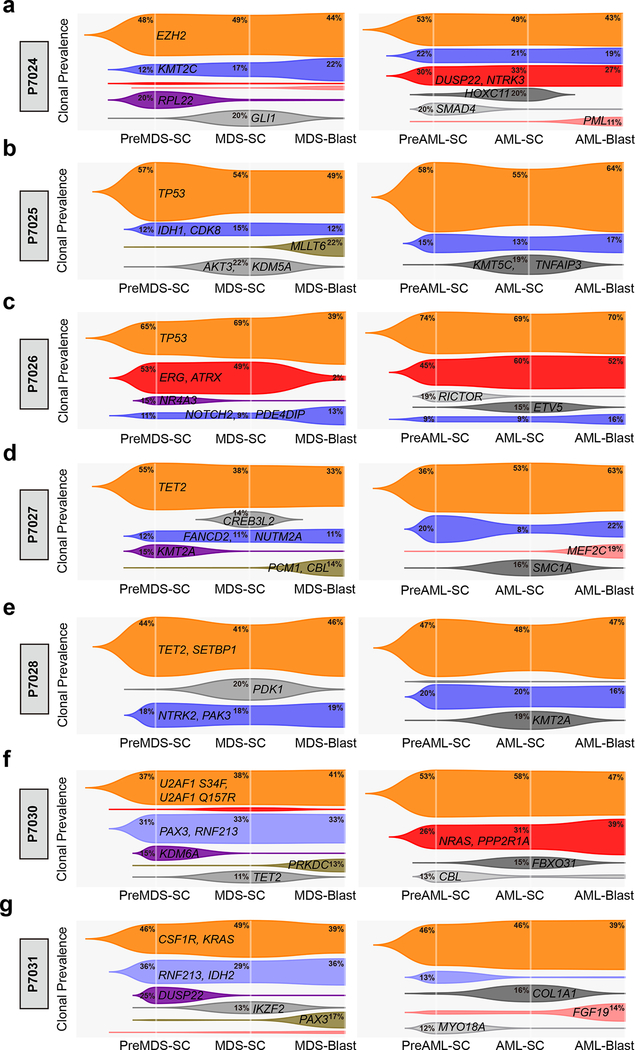
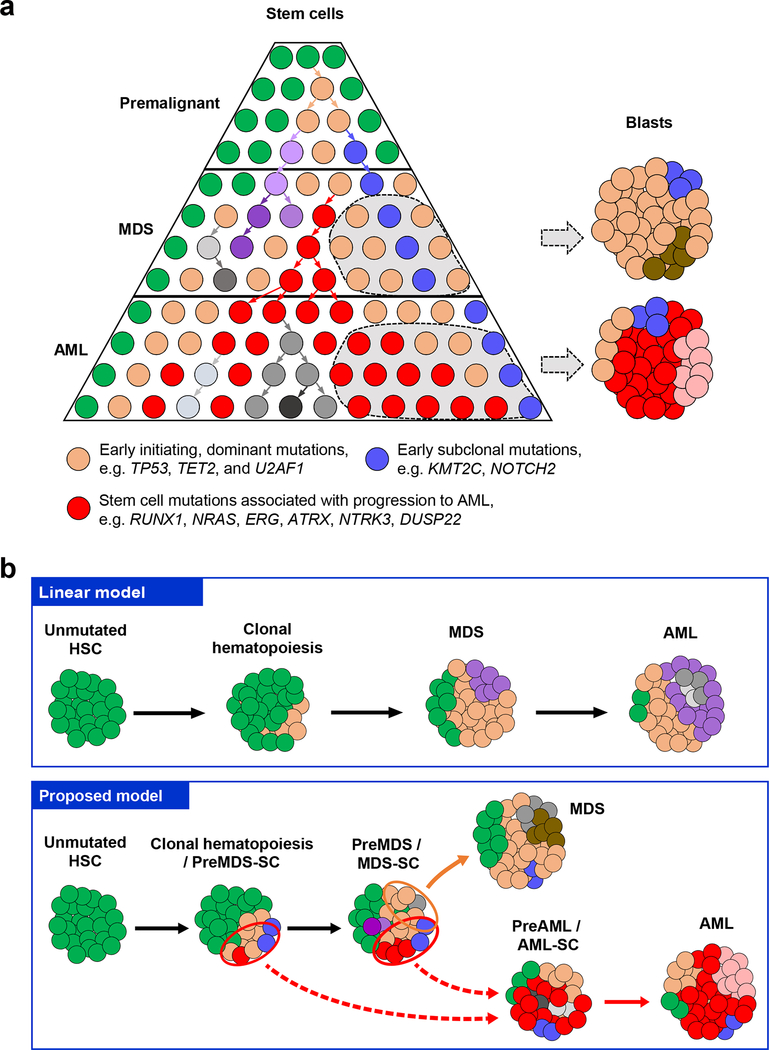
Myelodysplastic syndromes (MDS) frequently progress to acute myeloid leukemia (AML); however, the cells leading to malignant transformation have not been directly elucidated. As progression of MDS to AML in humans provides a biological system to determine the cellular origins and mechanisms of neoplastic transformation, we studied highly fractionated stem cell populations in longitudinal samples of patients with MDS who progressed to AML. Targeted deep sequencing combined with single-cell sequencing of sorted cell populations revealed that stem cells at the MDS stage, including immunophenotypically and functionally defined pre-MDS stem cells (pre-MDS-SC), had a significantly higher subclonal complexity compared to blast cells and contained a large number of aging-related variants. Single-cell targeted resequencing of highly fractionated stem cells revealed a pattern of nonlinear, parallel clonal evolution, with distinct subclones within pre-MDS-SC and MDS-SC contributing to generation of MDS blasts or progression to AML, respectively. Furthermore, phenotypically aberrant stem cell clones expanded during transformation and stem cell subclones that were not detectable in MDS blasts became dominant upon AML progression. These results reveal a crucial role of diverse stem cell compartments during MDS progression to AML and have implications for current bulk cell-focused precision oncology approaches, both in MDS and possibly other cancers that evolve from premalignant conditions, that may miss pre-existing rare aberrant stem cells that drive disease progression and leukemic transformation.
Figures

References
-
- Ades L, Itzykson R & Fenaux P Myelodysplastic syndromes. Lancet 383, 2239–2252 (2014). - PubMed
-
- Fialkow PJ, et al. Clonal Development, Stem-Cell Differentiation, and Clinical Remissions in Acute Nonlymphocytic Leukemia. New Engl J Med 317, 468–473 (1987). - PubMed
-
- Nilsson L, et al. Involvement and functional impairment of the CD34(+)CD38(−)Thy-1(+) hematopoietic stem cell pool in myelodysplastic syndromes with trisomy 8. Blood 100, 259–267 (2002). - PubMed
-
- Steidl U, et al. Essential role of Jun family transcription factors in PU.1 knockdown-induced leukemic stem cells. Nat Genet 38, 1269–1277 (2006). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
