

Low plasma haptoglobin is a risk factor for life-threatening childhood severe malarial anemia and not an exclusive consequence of hemolysis
- PMID: 30510258
- PMCID: PMC6277387
- DOI: 10.1038/s41598-018-35944-w
Low plasma haptoglobin is a risk factor for life-threatening childhood severe malarial anemia and not an exclusive consequence of hemolysis
Abstract
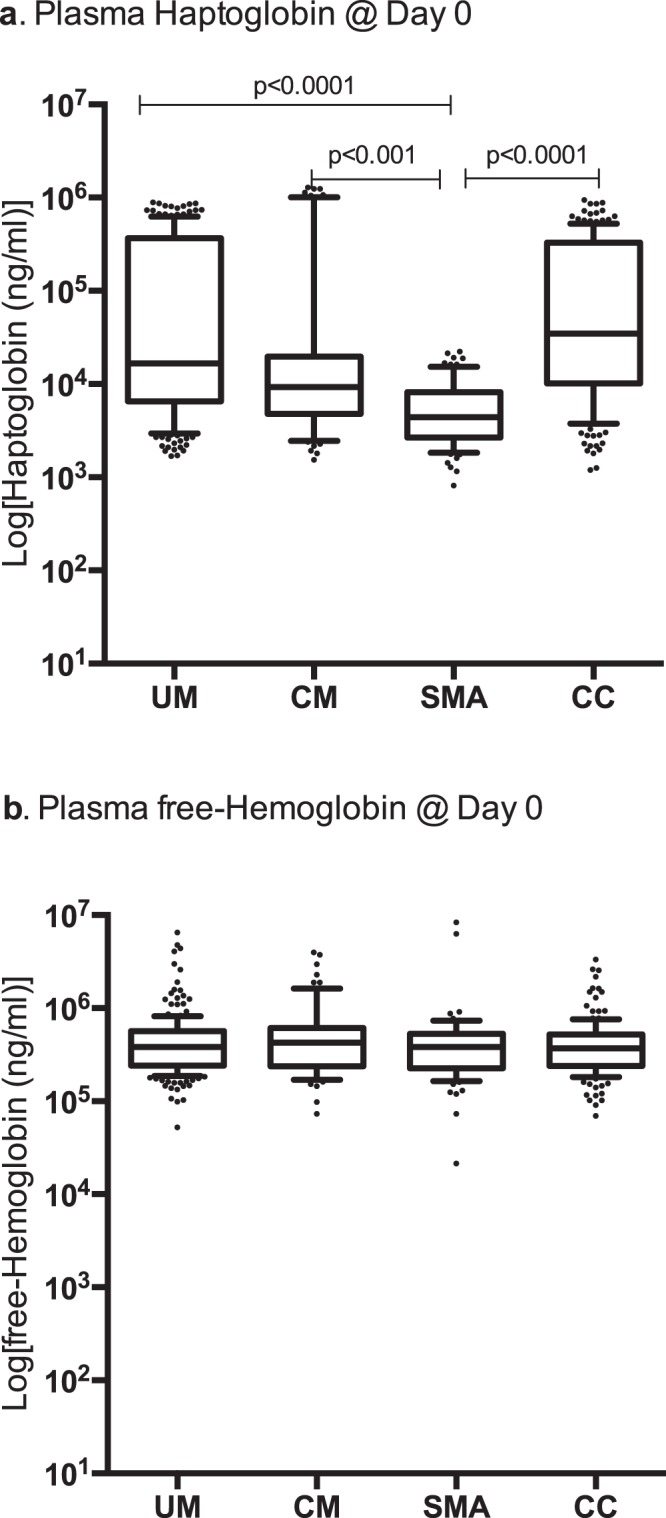
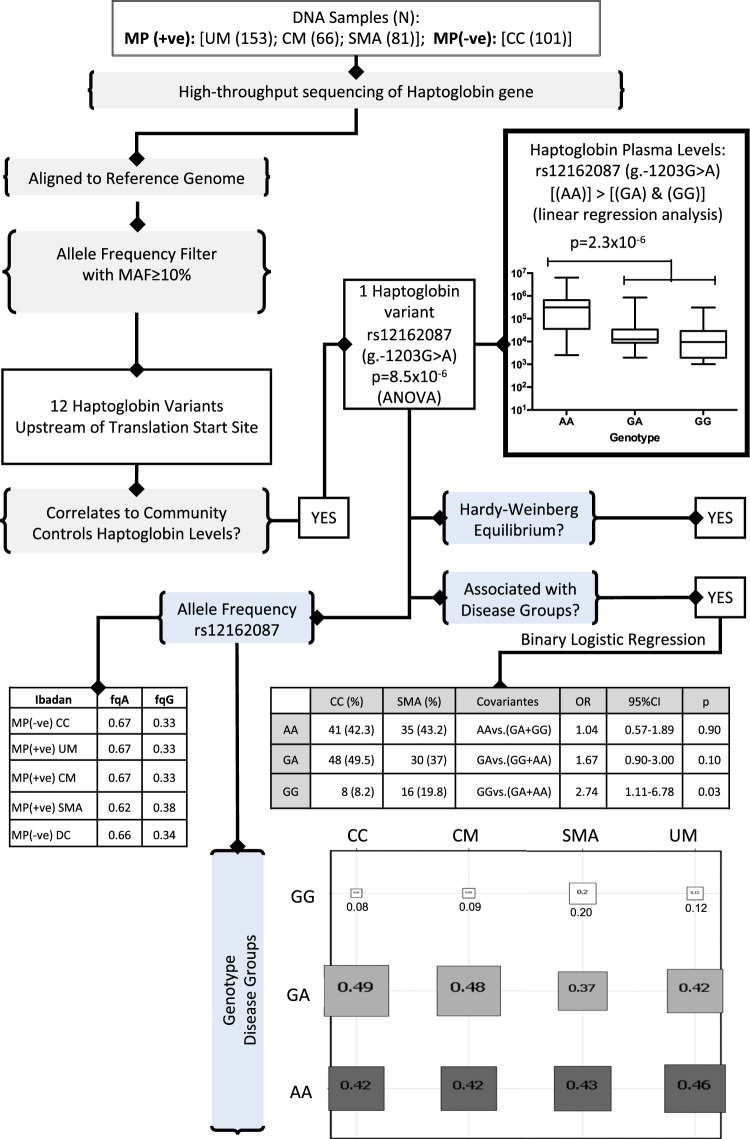
Severe Malarial Anemia (SMA), a life-threatening childhood Plasmodium falciparum malaria syndrome requiring urgent blood transfusion, exhibits inflammatory and hemolytic pathology. Differentiating between hypo-haptoglobinemia due to hemolysis or that of genetic origin is key to understand SMA pathogenesis. We hypothesized that while malaria-induced hypo-haptoglobinemia should reverse at recovery, that of genetic etiology should not. We carried-out a case-control study of children living under hyper-endemic holoendemic malaria burden in the sub-Saharan metropolis of Ibadan, Nigeria. We show that hypo-haptoglobinemia is a risk factor for childhood SMA and not solely due to intravascular hemolysis from underlying schizogony. In children presenting with SMA, hypo-haptoglobinemia remains through convalescence to recovery suggesting a genetic cause. We identified a haptoglobin gene variant, rs12162087 (g.-1203G > A, frequency = 0.67), to be associated with plasma haptoglobin levels (p = 8.5 × 10-6). The Homo-Var:(AA) is associated with high plasma haptoglobin while the reference Homo-Ref:(GG) is associated with hypo-haptoglobinemia (p = 2.3 × 10-6). The variant is associated with SMA, with the most support for a risk effect for Homo-Ref genotype. Our insights on regulatory haptoglobin genotypes and hypo-haptoglobinemia suggest that haptoglobin screening could be part of risk-assessment algorithms to prevent rapid disease progression towards SMA in regions with no-access to urgent blood transfusion where SMA accounts for high childhood mortality rates.
Conflict of interest statement
The authors declare no competing interests.
Figures


References
-
- World Health Organization. World Malaria Report 2017. doi:CC BY-NC-SA 3.0 IGO (World Health Organization, 2017).
-
- World Health Organization. World Malaria Report 2016. World Malaria Report doi:CC BY-NC-SA 3.0 IGO (World Health Organization, 2016).
-
- Ajetunmobi Wasiu A, Orimadegun Adebola E, Brown Biobele J, Afolabi Nathaniel K, Olabiyi Folorunso A, Anetor John I, Omokhodion Samuel, Osinusi Kikelomo, Akinbami Felix O, Shokunbi Wuraola A, Sodeinde Olugbemiro, Fernandez-Reyes Delmiro. Haemoglobinuria among children with severe malaria attending tertiary care in Ibadan, Nigeria. Malaria Journal. 2012;11(1):336. doi: 10.1186/1475-2875-11-336. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
