

Coronary spasm: It's common, but it's still unsolved
- PMID: 30510637
- PMCID: PMC6259026
- DOI: 10.4330/wjc.v10.i11.201
Coronary spasm: It's common, but it's still unsolved
Abstract
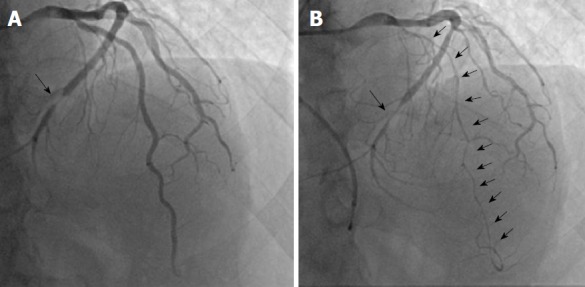
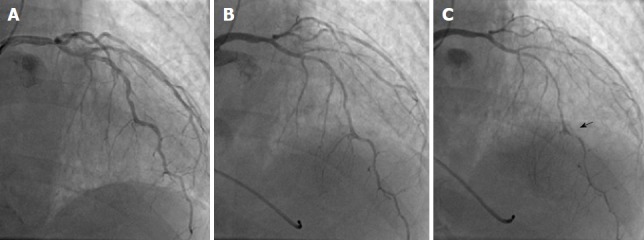
Coronary spasm is caused by a transient coronary narrowing due to the constriction of epicardial coronary artery, which leads to myocardial ischemia. More than 50 years have passed since the first recognition of coronary spasm, and many findings on coronary spasm have been reported. Coronary spasm has been considered as having pivotal roles in the cause of not only rest angina but also exertional angina, acute coronary syndrome, and heart failure. In addition, several new findings of the mechanism of coronary spasm have emerged recently. The diagnosis based mainly on coronary angiography and spasm provocation test and the mainstream treatment with a focus on a calcium-channel blocker have been established. At a glance, coronary spasm or vasospastic angina (VSA) has become a common disease. On the contrary, there are several uncertain or unsolved problems regarding coronary spasm, including the presence of medically refractory coronary spasm (intractable VSA), or an appropriate use of implantable cardioverter defibrillator in patients with cardiac arrest who have been confirmed as having coronary spasm. This editorial focused on coronary spasm, including recent topics and unsolved problems.
Keywords: Coronary vasospasm; Medically refractory coronary spasm; Variant angina; Vasospastic angina.
Conflict of interest statement
Conflict-of-interest statement: No potential conflict of interest. No financial support.
Figures
References
-
- Spritzler R, Corday E, Bergman HC, Prinzmetal M. Studies on the coronary circulation. VIII. Demonstration of spasm of the major coronary arteries. Cardiologia. 1952;21:255–258. - PubMed
-
- Prinzmetal M, Ekmekci A, Toyoshima H, Kwoczynski JK. Angina pectoris. III. Demonstration of a chemical origin of ST deviation in classic angina pectoris, its variant form, early myocardial infarction, and some noncardiac conditions. Am J Cardiol. 1959;3:276–293. - PubMed
-
- Prinzmetal M, Kennamer R, Merliss R, Wada T, Bor N. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am J Med. 1959;27:375–388. - PubMed
-
- Yasue H, Nagao M, Omote S, Takizawa A, Miwa K, Tanaka S. Coronary arterial spasm and Prinzmetal’s variant form of angina induced by hyperventilation and Tris-buffer infusion. Circulation. 1978;58:56–62. - PubMed
-
- Yasue H, Omote S, Takizawa A, Nagao M. Coronary arterial spasm in ischemic heart disease and its pathogenesis. A review. Circ Res. 1983;52:I147–I152. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
