

Dihydrotestosterone is a predictor for mortality in males with community-acquired pneumonia: results of a 6-year follow-up study
- PMID: 30514319
- PMCID: PMC6280517
- DOI: 10.1186/s12931-018-0947-0
Dihydrotestosterone is a predictor for mortality in males with community-acquired pneumonia: results of a 6-year follow-up study
Abstract
Background: Adrenal hormone metabolite levels are altered in acute illnesses such as community-acquired pneumonia (CAP). Our aim was to investigate associations of sex and mineralocorticoid hormone metabolites with short- and long-term mortality and severity of CAP in male and female patients.
Methods: We prospectively followed 285 patients (60.4% male, mean age 71 years) with CAP from a previous multicenter trial. At baseline, levels of different metabolites of sex hormones and mineralocorticoids were measured by liquid chromatography coupled to tandem mass spectrometry. We calculated Cox regression models adjusted for age and comorbidities.
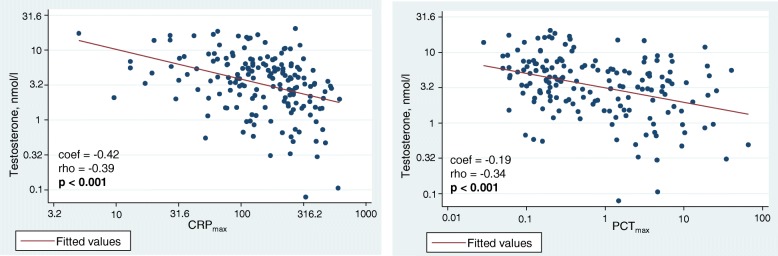
Results: All-cause mortality was 5.3% after 30 days and increased to 47.4% after 6 years. In males, high levels of dihydrotestosterone were associated with higher 6-year mortality (adjusted HR 2.84, 95%CI 1.15-6.99, p = 0.023), whereas high levels of 17-OH-progesterone were associated with lower 6-year mortality (adjusted HR 0.72, 95%CI 0.54-0.97, p = 0.029). Testosterone levels in males correlated inversely with inflammatory markers (CRP rho = - 0.39, p < 0.001; PCT rho = - 0.34, p < 0.001) and disease severity as assessed by the Pneumonia severity index (PSI) (rho = - 0.23, p = 0.003). No similar association was found for female patients.
Conclusion: Whereas in males with CAP, sex and mineralocorticoid hormone metabolite levels correlated with inflammation, disease severity and long-term survival, no similar association was found for females. Further study of sex and mineralocorticoid hormones in acute illness could generate predictive signatures with implementation in clinical practice.
Keywords: Adrenal hormones; Community-acquired pneumonia; Dihydrotestosterone; Mortality prediction.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the ethics committee of the University of Basel as well as by the local ethics committees of Aarau, Muensterlingen, Solothurn and Luzern, all with the same ethical study number 87/06. Written informed consent was provided by all participants for the initial trial, including agreement to use their data anonymized in secondary analyses.
Consent for publication
Not applicable.
Competing interests
All authors declare that they have no competing interests associated with this manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Mortality GBD, Causes of death C. global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980-2015: a systematic analysis for the global burden of disease study 2015. Lancet (London, England) 2016;388(10053):1459–544. - PMC - PubMed
-
- Kolditz M, Hoffken G, Martus P, Rohde G, Schutte H, Bals R, et al. Serum cortisol predicts death and critical disease independently of CRB-65 score in community-acquired pneumonia: a prospective observational cohort study. BMC Infect Dis. 2012;12:90. doi: 10.1186/1471-2334-12-90. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
