

Miscarriage Treatment-Related Morbidities and Adverse Events in Hospitals, Ambulatory Surgery Centers, and Office-Based Settings
- PMID: 30516583
- PMCID: PMC7678655
- DOI: 10.1097/PTS.0000000000000553
Miscarriage Treatment-Related Morbidities and Adverse Events in Hospitals, Ambulatory Surgery Centers, and Office-Based Settings
Abstract
Objective: The aim of the study was to examine whether miscarriage treatment-related morbidities and adverse events vary across facility types.
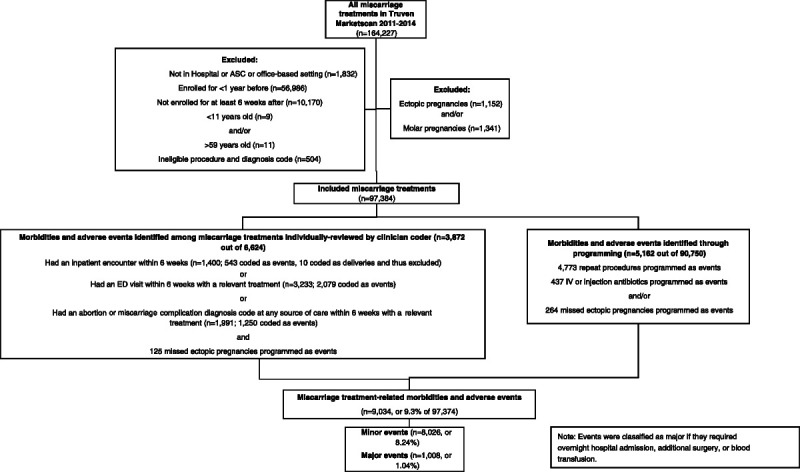
Methods: A retrospective cohort study compared miscarriage treatment-related morbidities and adverse events across hospitals, ambulatory surgery centers (ASCs), and office-based settings. Data on women who had miscarriage treatment between 2011 and 2014 and were continuously enrolled in their insurance plan for at least 1 year before and at least 6 weeks after treatment were obtained from a large national private insurance claims database. The main outcome was miscarriage treatment-related morbidities and adverse events occurring within 6 weeks of miscarriage treatment. Secondary outcomes were major events and infections.
Results: A total of 97,374 miscarriage treatments met inclusion criteria. Most (75%) were provided in hospitals, 10% ASCs, and 15% office-based settings. A total of 9.3% had miscarriage treatment-related events, 1.0% major events, and 1.5% infections. In adjusted analyses, there were fewer events in ASCs (6.5%) than office-based settings (9.4%) and hospitals (9.6%), but no significant difference between office-based settings and hospitals. There were no significant differences in major events between ASCs (0.7%) and office-based settings (0.8%), but more in hospitals (1.1%) than ASCs and office-based settings. There were fewer infections in ASCs (0.9%) than office-based settings (1.2%) and more in hospitals (1.6%) than ASCs and office-based settings. In analyses stratified by miscarriage treatment type, the difference between ASCs and office-based settings was no longer significant for miscarriages treated with procedures.
Conclusions: Although there seem to be slightly more events in hospitals than ASCs or office-based settings, findings do not support limiting miscarriage treatment to particular settings.
Conflict of interest statement
The authors report no conflict of interest.
Similar articles
-
Association of Facility Type With Procedural-Related Morbidities and Adverse Events Among Patients Undergoing Induced Abortions.JAMA. 2018 Jun 26;319(24):2497-2506. doi: 10.1001/jama.2018.7675. JAMA. 2018. PMID: 29946727 Free PMC article.
-
Healthcare costs for abortions performed in ambulatory surgery centers vs office-based settings.Am J Obstet Gynecol. 2020 Apr;222(4):348.e1-348.e9. doi: 10.1016/j.ajog.2019.10.002. Epub 2019 Oct 17. Am J Obstet Gynecol. 2020. PMID: 31629727
-
Comparison of Safety and Insurance Payments for Minor Hand Procedures Across Operative Settings.JAMA Netw Open. 2020 Oct 1;3(10):e2015951. doi: 10.1001/jamanetworkopen.2020.15951. JAMA Netw Open. 2020. PMID: 33048128 Free PMC article.
-
Ambulatory surgery centers and interventional techniques: a look at long-term survival.Pain Physician. 2011 Mar-Apr;14(2):E177-215. Pain Physician. 2011. PMID: 21412380 Review.
-
Progestogen for preventing miscarriage in women with recurrent miscarriage of unclear etiology.Cochrane Database Syst Rev. 2018 Oct 8;10(10):CD003511. doi: 10.1002/14651858.CD003511.pub4. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2019 Nov 20;2019(11). doi: 10.1002/14651858.CD003511.pub5. PMID: 30298541 Free PMC article. Updated.
Cited by
-
What organisational and regional factors influence the outpatient provision of curettages in Germany? A longitudinal secondary data analysis using hospital quality reports data from 2013 to 2019.BMJ Open. 2023 Oct 6;13(10):e072887. doi: 10.1136/bmjopen-2023-072887. BMJ Open. 2023. PMID: 37802629 Free PMC article.
-
Early Pregnancy Loss Management in the Emergency Department vs Outpatient Setting.JAMA Netw Open. 2023 Mar 1;6(3):e232639. doi: 10.1001/jamanetworkopen.2023.2639. JAMA Netw Open. 2023. PMID: 36920395 Free PMC article.
References
-
- Cullen KA, Hall MJ, Golosinskiy A. Ambulatory surgery in the United States, 2006. Natl Health Stat Report. 2009;1–25. - PubMed
-
- Harris LH, Dalton VK, Johnson TR. Surgical management of early pregnancy failure: history, politics, and safe, cost-effective care. Am J Obstet Gynecol. 2007;196:445.e1–445.e5. - PubMed
-
- Hollingsworth JM Birkmeyer JD Ye Z, et al. . Specialty-specific trends in the prevalence and distribution of outpatient surgery: implications for payment and delivery system reforms. Surg Innov. 2014;21:560–565. - PubMed
-
- Dalton VK Liang A Hutton DW, et al. . Beyond usual care: the economic consequences of expanding treatment options in early pregnancy loss. Am J Obstet Gynecol. 2015;212:177.e1–177.e6. - PubMed
-
- Dalton VK Harris L Weisman CS, et al. . Patient preferences, satisfaction, and resource use in office evacuation of early pregnancy failure. Obstet Gynecol. 2006;108:103–110. - PubMed
