

Proposal for a New Histological Scoring System for Cartilage Repair
- PMID: 30517286
- PMCID: PMC6238816
- DOI: 10.6061/clinics/2018/e562
Proposal for a New Histological Scoring System for Cartilage Repair
Abstract
Objective: This study aimed to develop a new histological scoring system for use in a partial-thickness cartilage repair animal model. Although previous papers have investigated the regeneration of articular cartilage, the good results achieved in small animals have not been replicated in large animal models or humans, possibly because of the frequent use of models with perforation of the subchondral bone plates. Partial-thickness lesions spare the subchondral bone, and this pattern is the most frequent in humans; therefore, new therapies should be tested using this model. However, no specific histological score exists to evaluate partial-thickness model results.
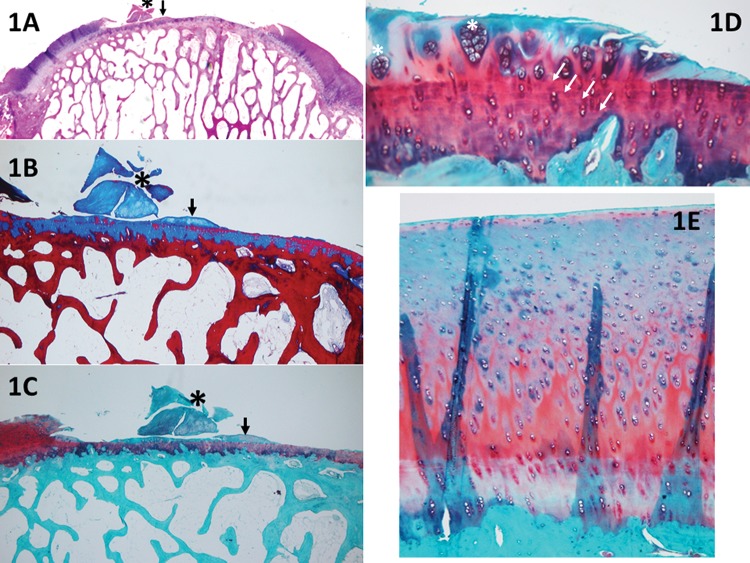
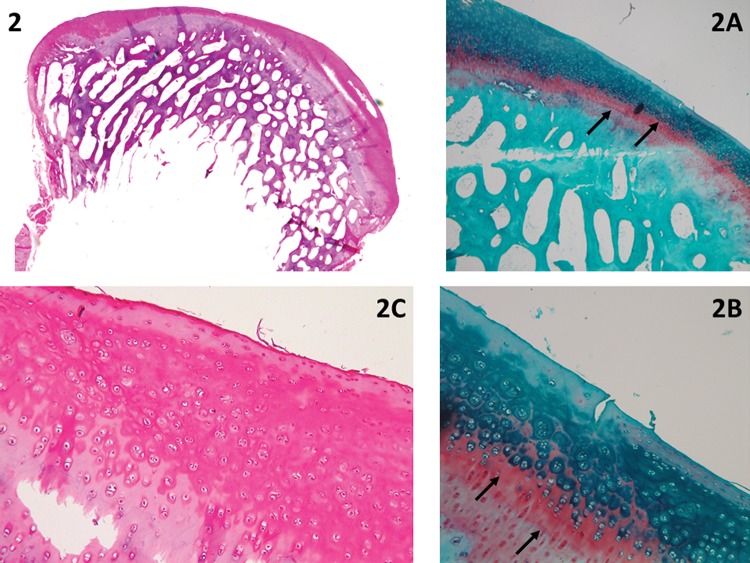
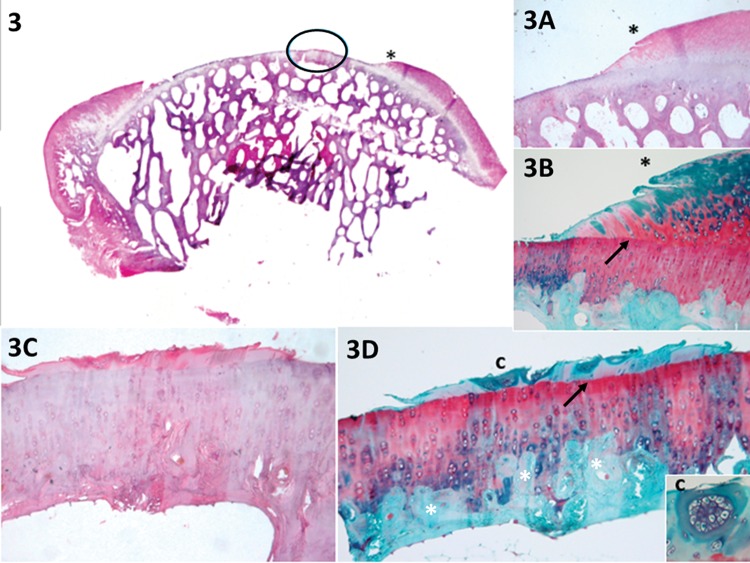
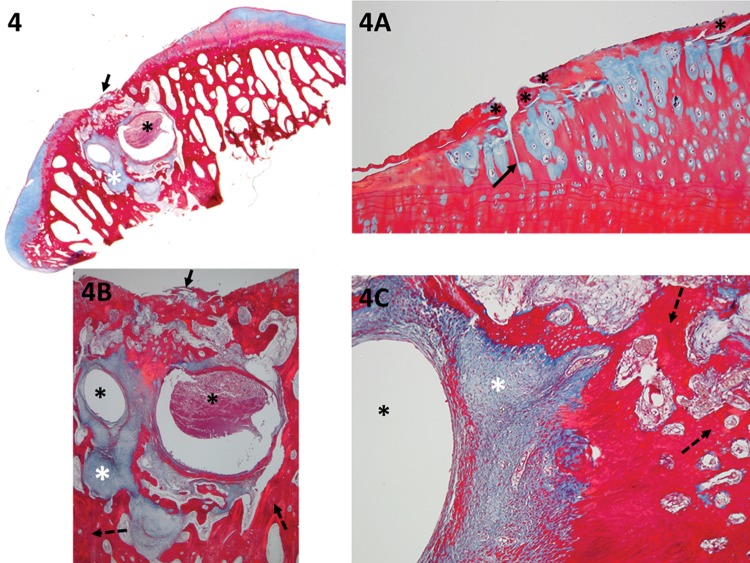
Methods: Histological sections from 30 ovine knees were reviewed to develop a new scoring system. The sections were subjected to H&E, Safranin O, and Masson's trichrome staining.
Results: This paper describes a new scoring tool that is divided into sections in detail: repair of tissue inside the lesion, cartilage around the lesion and degenerative changes at the base of the lesion. Scores range from 0 to 21; a higher score indicates better cartilage repair.
Discussion: Unlike existing tools, this new scale does not assign points for the positioning of a tidemark; we propose evaluation of the degenerative changes to the subchondral bone and calcified cartilage layer. It is necessary to remove the whole joint to access and study the evolution of the lesion as well as the surrounding tissue.
Conclusion: This article emphasizes the importance of a partial-thickness animal model of cartilage repair and presents a new histological scoring system.
Conflict of interest statement
No potential conflict of interest was reported.
Figures
References
-
- Saris DB, Vanlauwe J, Victor J, Haspl M, Bohnsack M, Fortems Y, et al. Characterized chondrocyte implantation results in better structural repair when treating symptomatic cartilage defects of the knee in a randomized controlled trial versus microfracture. Am J Sports Med. 2008;36((2)):235–46. doi: 10.1177/0363546507311095. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
