

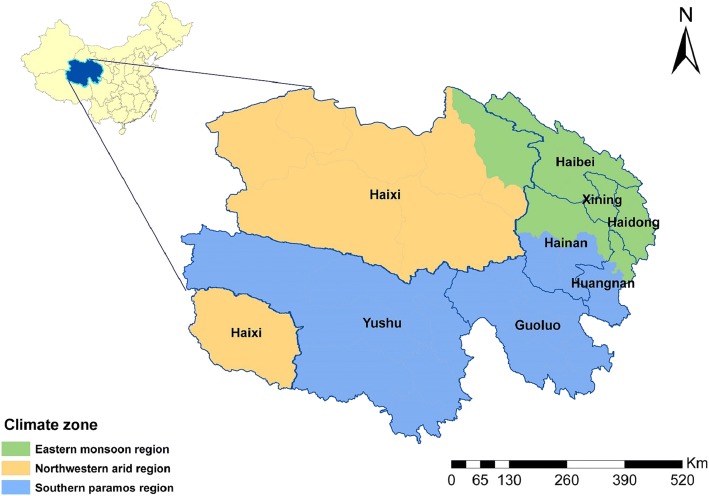
Epidemiological features and spatial clusters of hand, foot, and mouth disease in Qinghai Province, China, 2009-2015
- PMID: 30518329
- PMCID: PMC6280489
- DOI: 10.1186/s12879-018-3509-7
Epidemiological features and spatial clusters of hand, foot, and mouth disease in Qinghai Province, China, 2009-2015
Abstract
Background: Hand, Foot, and Mouth Disease (HFMD) is most frequently caused by Enterovirus71 (EV-A71) or Coxsackie virus A16 (CV-A16), infants and young children are at greatest risk. Describing the epidemiology of HFMD can help develop and better target interventions, including the use of pediatric EV-A71 vaccination.
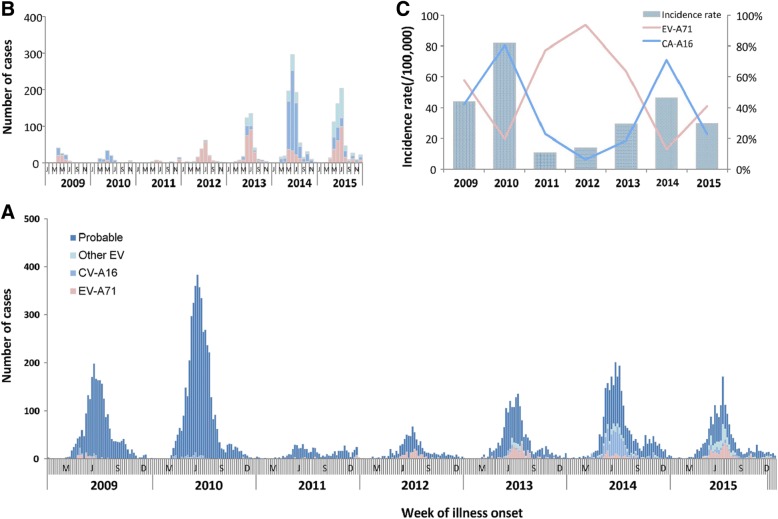
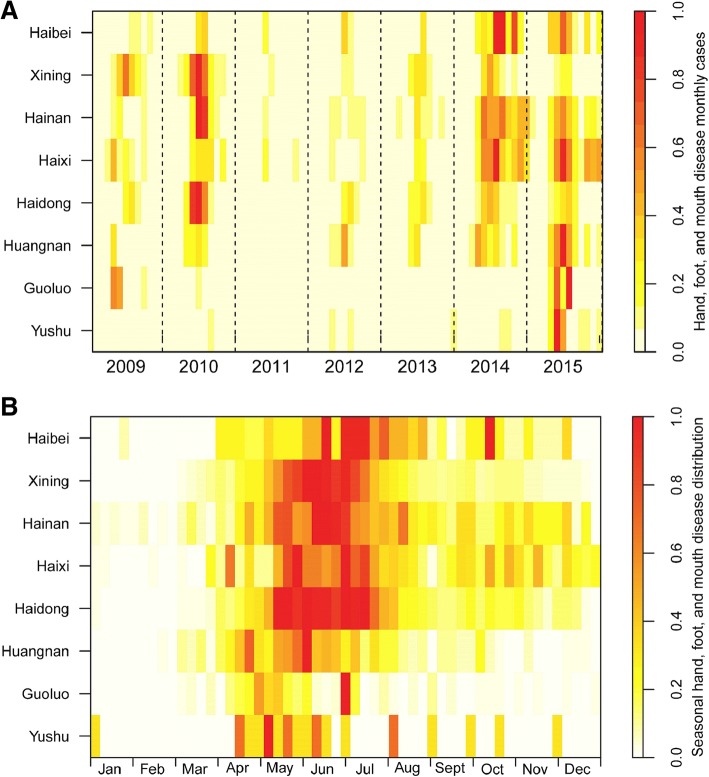
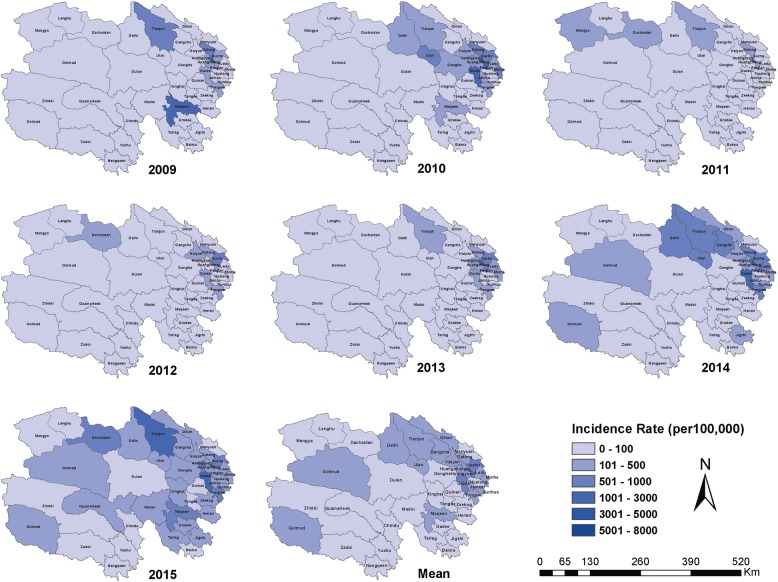
Methods: We obtained data from the national surveillance system for HFMD cases with onset dates from 2009 to 2015. We defined probable cases as patient with skin papular or vesicular rashes on the hands, feet, mouth, or buttocks and confirmed cases as patients with the above symptoms along with laboratory-based enterovirus detection. We generated overall and age-specific annual incidence rates and described the temporal variability and seasonality of HFMD in Qinghai Province. We identified spatial clustering of HFMD incidence at the county level using the Local Indicator of Spatial Associationand an alpha level of 0.05.
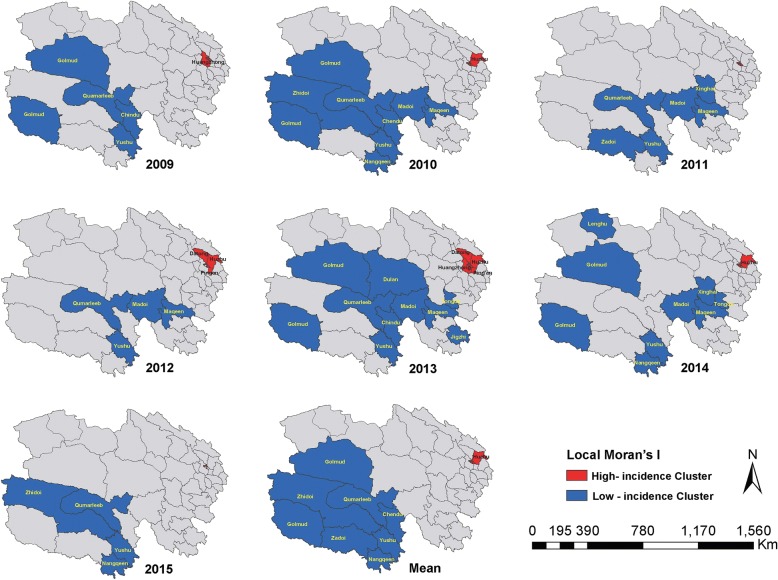
Results: During the study period, 14,480 HFMD probable or confirmed cases were reported in Qinghai Province. Of the 2158 (14.9%) with laboratory confirmation, 924 (42.6%) were caused by CV-A16 and 830 (38.2%) were caused by EV-A71. The majority (89%) of all case-patients were ≤ 5 years of age and male (61.5%). The overall mean annual HFMD incidence rate was 36.4 cases per 100,000 populations, while the incidence rate for children ≤5 years of age was 379.5 cases per 100,000. Case reports peaked during the months of May through July. HFMD was predominantly caused by EV-A71, except in 2010 and 2014 when CV-A16 was the predominant causative agent. High incidence rates of HFMD were clustered (Moran's I = 0.59, P < 0.05) in the eastern region of the province.
Conclusion: HFMD remains an important cause of childhood disease in Qinghai Province, occurring in an acyclical pattern of increased incidence, primarily due to CV-A16 circulation every three years. Incidence is also seasonal and tends to spatially cluster in the eastern region of the province. Since approximately 40% of confirmed HFMD cases were due to EV-A71, EV-A71 vaccination is likely to have a positive impact on the HFMD disease burden. Routine analysis of local surveillance data is crucial for describing disease occurrence and changes in etiology.
Keywords: Cyclical pattern; HFMD; Qinghai Province; Spatial clusters.
Conflict of interest statement
Ethics approval and consent to participate
According to the National Health Commission of China, the national surveillance protocol for HFMD is part of an ongoing public health response and, therefore, exempt from review by Qinghai’s CDC IRB. The United States Centers for Disease Control and Prevention approved the project as a routine surveillance activity. Personal identifying information such as patient name, parent name, home address, and telephone number were deleted prior to analysis.
Consent for publication
Not applicable.
Competing interests
We declare that we have no conflicts of interest.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Hand, Foot, and Mouth Disease in China: Modeling Epidemic Dynamics of Enterovirus Serotypes and Implications for Vaccination.PLoS Med. 2016 Feb 16;13(2):e1001958. doi: 10.1371/journal.pmed.1001958. eCollection 2016 Feb. PLoS Med. 2016. PMID: 26882540 Free PMC article.
-
[Analysis on epidemiological characteristics of enterovirus 71 cases of hand-foot-mouth disease based on the active monitoring in Guangdong Province in 2011-2015].Zhonghua Yu Fang Yi Xue Za Zhi. 2018 Jul 6;52(7):738-742. doi: 10.3760/cma.j.issn.0253-9624.2018.07.011. Zhonghua Yu Fang Yi Xue Za Zhi. 2018. PMID: 29996302 Chinese.
-
Epidemiological Characteristics and Spatial-Temporal Clusters of Hand, Foot, and Mouth Disease in Zhejiang Province, China, 2008-2012.PLoS One. 2015 Sep 30;10(9):e0139109. doi: 10.1371/journal.pone.0139109. eCollection 2015. PLoS One. 2015. PMID: 26422015 Free PMC article.
-
Is a multivalent hand, foot, and mouth disease vaccine feasible?Hum Vaccin Immunother. 2015;11(11):2688-704. doi: 10.1080/21645515.2015.1049780. Epub 2015 May 26. Hum Vaccin Immunother. 2015. PMID: 26009802 Free PMC article. Review.
-
Enterovirus-Associated Hand-Foot and Mouth Disease and Neurological Complications in Japan and the Rest of the World.Int J Mol Sci. 2019 Oct 20;20(20):5201. doi: 10.3390/ijms20205201. Int J Mol Sci. 2019. PMID: 31635198 Free PMC article. Review.
Cited by
-
Epidemiological characteristics and spatial-temporal clusters of hand, foot, and mouth disease in Qingdao City, China, 2013-2018.PLoS One. 2020 Jun 5;15(6):e0233914. doi: 10.1371/journal.pone.0233914. eCollection 2020. PLoS One. 2020. PMID: 32502174 Free PMC article.
-
Epidemiological characteristics, spatial clusters and monthly incidence prediction of hand, foot and mouth disease from 2017 to 2022 in Shanxi Province, China.Epidemiol Infect. 2023 Mar 14;151:e54. doi: 10.1017/S0950268823000389. Epidemiol Infect. 2023. PMID: 37039461 Free PMC article.
-
Research on hand, foot and mouth disease incidence forecasting using hybrid model in mainland China.BMC Public Health. 2023 Mar 31;23(1):619. doi: 10.1186/s12889-023-15543-9. BMC Public Health. 2023. PMID: 37003988 Free PMC article.
-
Nonlinear effect of temperature on hand, foot, and mouth disease in Lanzhou, China.Medicine (Baltimore). 2020 Nov 6;99(45):e23007. doi: 10.1097/MD.0000000000023007. Medicine (Baltimore). 2020. PMID: 33157945 Free PMC article.
-
Temporal and Spatial Cluster Analysis of 2019 Novel Coronavirus Pneumonia in Chongqing, 2020.1∼2020.2.Comput Intell Neurosci. 2022 Sep 16;2022:8491628. doi: 10.1155/2022/8491628. eCollection 2022. Comput Intell Neurosci. 2022. PMID: 36156965 Free PMC article.
References
-
- Kogon A, Spigland I, Frothingham TE, Elveback L, Williams C, Hall CE, Fox JP. The virus watch program: a continuing surveillance of viral infections in metropolitan New York families. VII. Observations on viral excretion, seroimmunity, intrafamilial spread and illness association in coxsackie and echovirus infections. Am J Epidemiol. 1969;94(1):367–385. - PubMed
-
- Zeng M, Khatib NFE, Tu S, Ren P, Xu S, Zhu Q, Mo X, Pu D, Wang X, Altmeyer R. Seroepidemiology of enterovirus 71 infection prior to the 2011 season in children in Shanghai. Journal of Clinical Virology the Official Publication of the Pan American Society for Clinical. Virology. 2012;53(4):285–289. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
