

Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study
- PMID: 30518517
- PMCID: PMC6278585
- DOI: 10.1136/bmj.k4764
Patient safety after implementation of a coproduced family centered communication programme: multicenter before and after intervention study
Abstract
Objective: To determine whether medical errors, family experience, and communication processes improved after implementation of an intervention to standardize the structure of healthcare provider-family communication on family centered rounds.
Design: Prospective, multicenter before and after intervention study.
Setting: Pediatric inpatient units in seven North American hospitals, 17 December 2014 to 3 January 2017.
Participants: All patients admitted to study units (3106 admissions, 13171 patient days); 2148 parents or caregivers, 435 nurses, 203 medical students, and 586 residents.
Intervention: Families, nurses, and physicians coproduced an intervention to standardize healthcare provider-family communication on ward rounds ("family centered rounds"), which included structured, high reliability communication on bedside rounds emphasizing health literacy, family engagement, and bidirectional communication; structured, written real-time summaries of rounds; a formal training programme for healthcare providers; and strategies to support teamwork, implementation, and process improvement.
Main outcome measures: Medical errors (primary outcome), including harmful errors (preventable adverse events) and non-harmful errors, modeled using Poisson regression and generalized estimating equations clustered by site; family experience; and communication processes (eg, family engagement on rounds). Errors were measured via an established systematic surveillance methodology including family safety reporting.
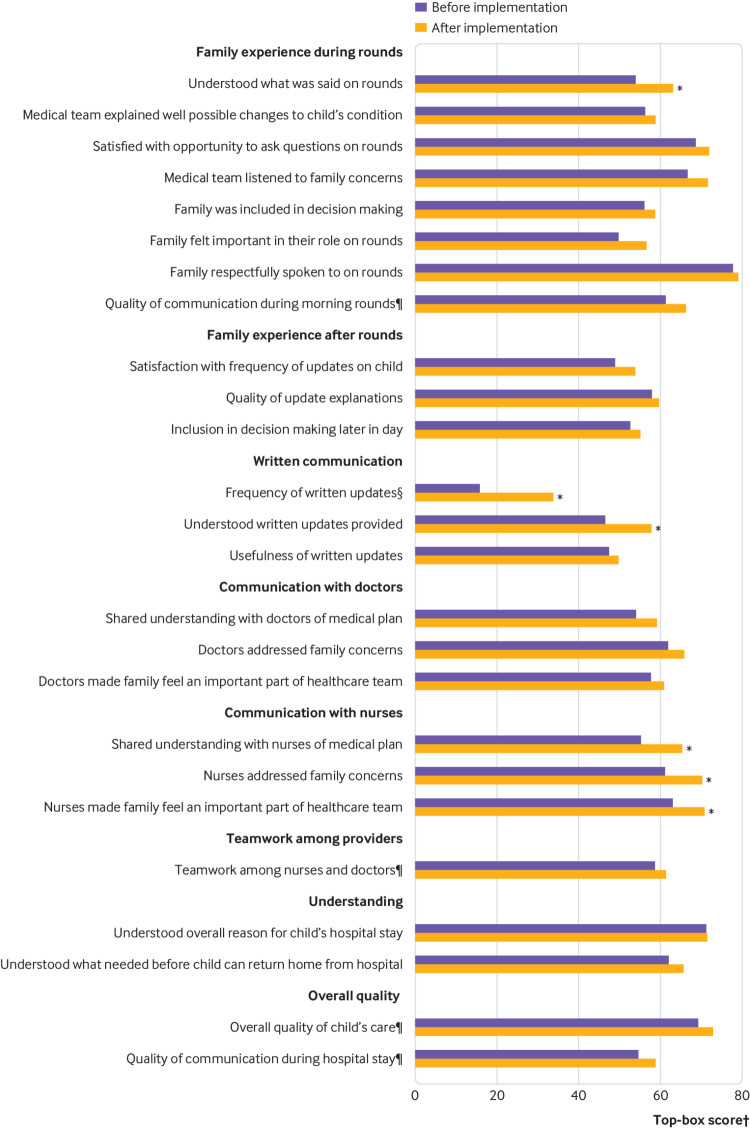
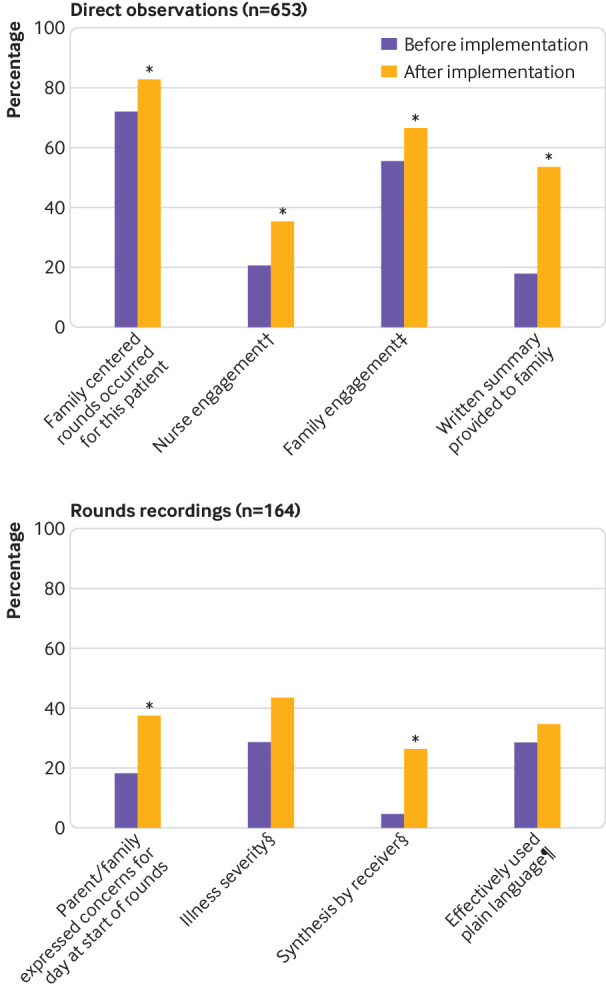
Results: The overall rate of medical errors (per 1000 patient days) was unchanged (41.2 (95% confidence interval 31.2 to 54.5) pre-intervention v 35.8 (26.9 to 47.7) post-intervention, P=0.21), but harmful errors (preventable adverse events) decreased by 37.9% (20.7 (15.3 to 28.1) v 12.9 (8.9 to 18.6), P=0.01) post-intervention. Non-preventable adverse events also decreased (12.6 (8.9 to 17.9) v 5.2 (3.1 to 8.8), P=0.003). Top box (eg, "excellent") ratings for six of 25 components of family reported experience improved; none worsened. Family centered rounds occurred more frequently (72.2% (53.5% to 85.4%) v 82.8% (64.9% to 92.6%), P=0.02). Family engagement 55.6% (32.9% to 76.2%) v 66.7% (43.0% to 84.1%), P=0.04) and nurse engagement (20.4% (7.0% to 46.6%) v 35.5% (17.0% to 59.6%), P=0.03) on rounds improved. Families expressing concerns at the start of rounds (18.2% (5.6% to 45.3%) v 37.7% (17.6% to 63.3%), P=0.03) and reading back plans (4.7% (0.7% to 25.2%) v 26.5% (12.7% to 7.3%), P=0.02) increased. Trainee teaching and the duration of rounds did not change significantly.
Conclusions: Although overall errors were unchanged, harmful medical errors decreased and family experience and communication processes improved after implementation of a structured communication intervention for family centered rounds coproduced by families, nurses, and physicians. Family centered care processes may improve safety and quality of care without negatively impacting teaching or duration of rounds.
Trial registration: ClinicalTrials.gov NCT02320175.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare no associations with commercial entities that provided support for the work reported in the submitted manuscript. JFB, AKD, CPL, SJP, TCS, SSS, NDS, AJS, and DCW hold equity in the I-PASS Patient Safety Institute. RS works for Intermountain Healthcare, which holds equity in the I-PASS Patient Safety Institute. SC, JKO’T, and SJP hold stock options in the I-PASS Patient Safety Institute. SC, CPL, JKO’T, SJP, GR, TCS, NDS, AJS, and DCW have consulted with the I-PASS Patient Safety Institute. The I-PASS Patient Safety Institute is a company that seeks to train institutions in best handoff practices and aid in their implementation. The current study was designed before the I-PASS Patient Safety Institute was conceived of as an entity and the I-PASS Patient Safety Institute is not involved in bedside rounds or family-centered care and was in no way involved in this study. Moreover, to ensure objectivity, all data were sent directly from the sites to the statistical team at the Data Coordinating Center, who do not have any involvement with the I-PASS Patient Safety Institute. All analyses were conducted by this statistical team. TCS, NDS, AJS, and DCW have received monetary awards, honorariums, and travel reimbursement from multiple academic and professional organizations for teaching and consulting on physician performance and handoffs. CPL and RS are supported in part by the Children’s Hospital Association for their work as executive council members of the Pediatric Research in Inpatient Settings (PRIS) network. RS has received monetary awards, honorariums, and travel reimbursement from multiple academic and professional organizations for talks about pediatric hospitalist research networks and quality of care. CPL has also served as a paid consultant to Virgin Pulse to help develop a Sleep and Health Program. In addition, CPL has received monetary awards, honoraria, and travel reimbursement from multiple academic and professional organizations for teaching and consulting on sleep deprivation, physician performance, handoffs, and safety, and has served as an expert witness in cases regarding patient safety and sleep deprivation. All other authors have no conflicts of interest to disclose at this time.
Figures
References
-
- Institute of Medicine . To Err is Human: Building a Safer Health System. The National Academies Press, 2000. - PubMed
-
- World Health Organization Regional Office for Europe. Data and statistics. www.euro.who.int/en/health-topics/Health-systems/patient-safety/data-and... (accessed 24 Oct 2018).
-
- World Health Organization Regional Office for Europe. A Brief Synopsis on Patient Safety. World Health Organization: Copenhagen, 2010. www.euro.who.int/en/health-topics/Health-systems/patient-safety/publicat....
-
- The Joint Commission. Sentinel event statistics released for 2014. Jt Comm Online 2015. www.jointcommission.org/assets/1/23/jconline_April_29_15.pdf (accessed 24 Oct 2018).
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical