

Rural and urban disparities in the care of Canadian patients with inflammatory bowel disease: a population-based study
- PMID: 30519110
- PMCID: PMC6233859
- DOI: 10.2147/CLEP.S178056
Rural and urban disparities in the care of Canadian patients with inflammatory bowel disease: a population-based study
Abstract
Background and aims: Canada's large geographic area and low population density pose challenges in access to specialized health care for remote and rural residents. We compared health services use, surgical rate, and specialist gastroenterologist care in rural and urban inflammatory bowel disease (IBD) patients in Canada.
Methods: We used validated algorithms that were applied to population-based health administrative data to identify all people living with the following three Canadian provinces: Alberta, Manitoba, and Ontario (ON). We compared rural residents with urban residents for time to diagnosis, hospitalizations, outpatient visits, emergency department (ED) use, surgical rate, and gastroenterologist care. Multivariable regression compared the outcomes in rural/urban patients, controlling for confounders. Provincial results were meta-analyzed using random-effects models to produce overall estimates.
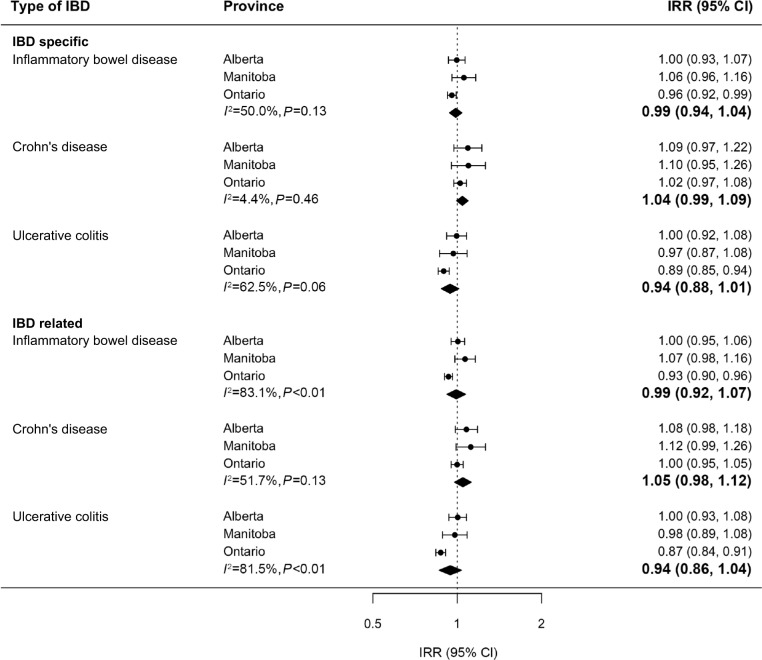
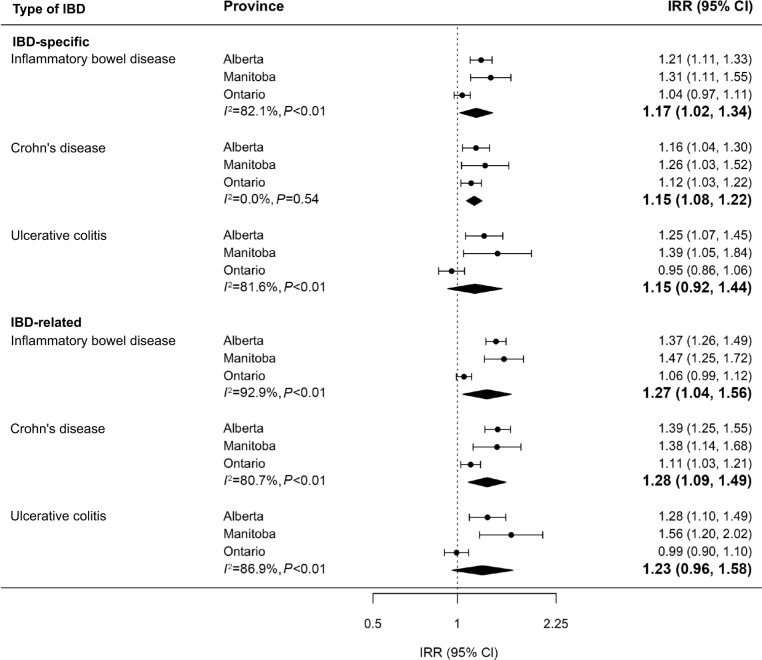
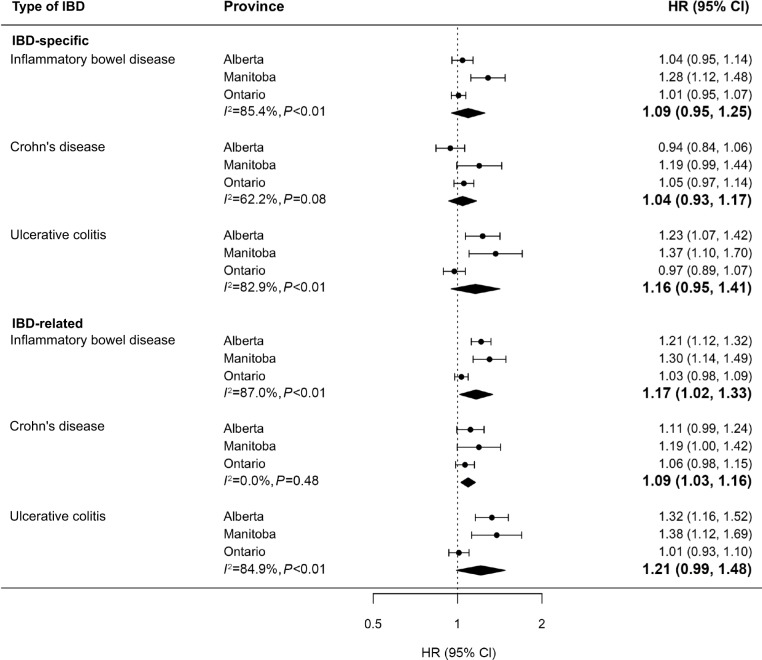
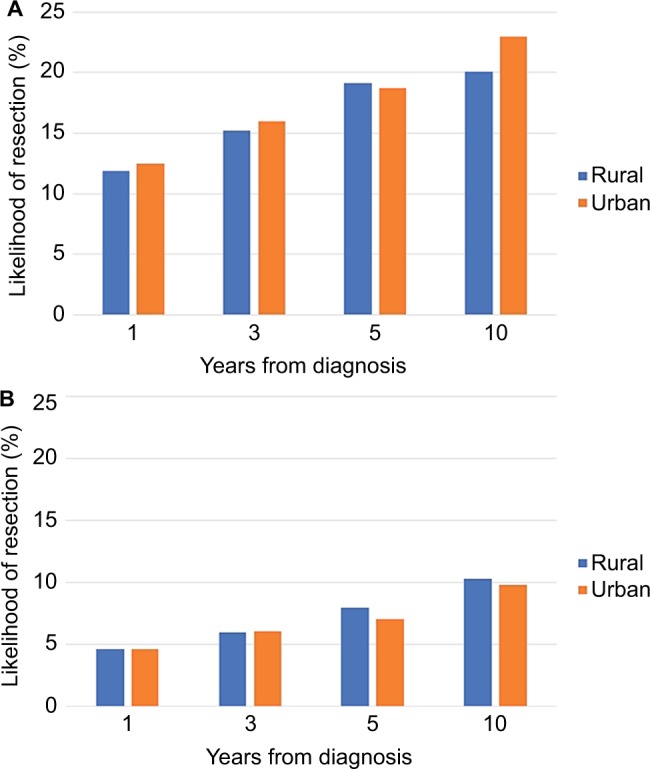
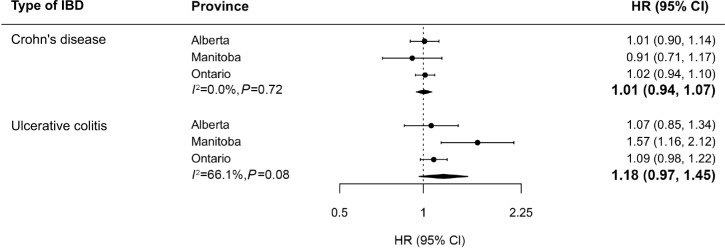
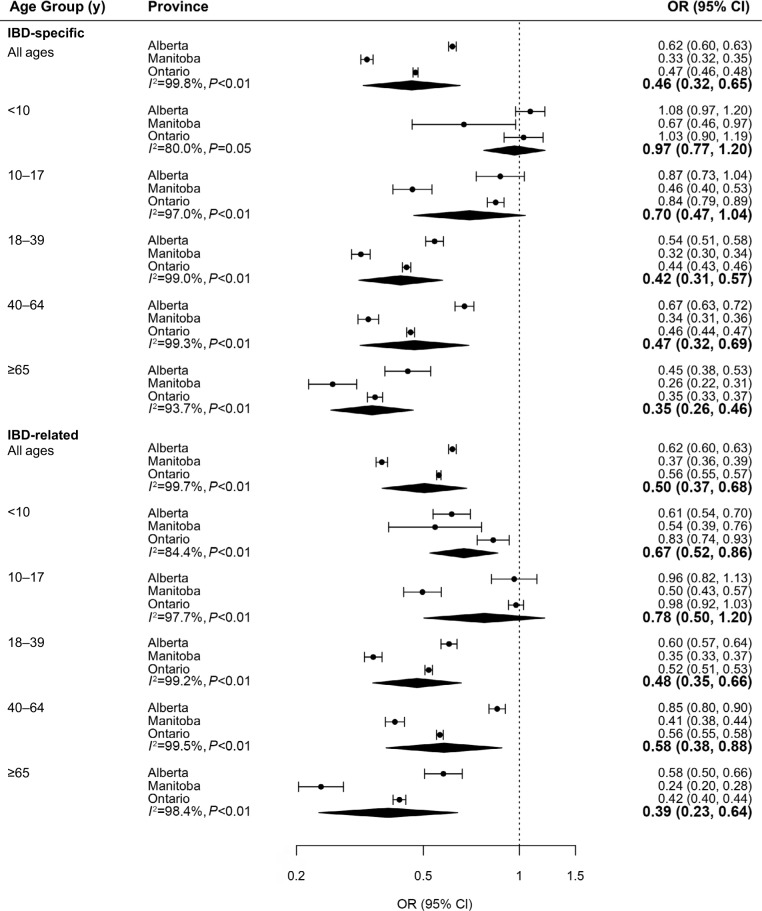
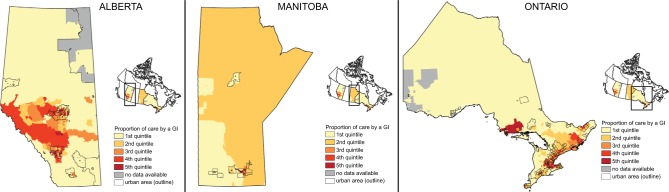
Results: A total of 36,656 urban and 5,223 rural residents with incident IBD were included. Outpatient physician visit rate was similar in rural and urban patients. IBD-specific and IBD-related hospitalization rates were higher in rural patients (incidence rate ratio [IRR] 1.17, 95% CI 1.02-1.34, and IRR 1.27, 95% CI 1.04-1.56, respectively). The rate of ED visits in ON were similarly elevated for rural patients (IRR 1.53, 95% CI 1.42-1.65, and IRR 1.33, 95% CI 1.25-1.40). There were no differences in surgical rates or prediagnosis lag time between rural and urban patients. Rural patients had fewer IBD-specific gastroenterologist visits (IRR 0.79, 95% CI 0.73-0.84) and a smaller proportion of their IBD-specific care was provided by gastroenterologists (28.3% vs 55.2%, P<0.0001). This was less pronounced in children <10 years at diagnosis (59.3% vs 65.0%, P<0.0001), and the gap was widest in patients >65 years (33.0% vs 59.2%, P<0.0001).
Conclusion: There were lower rates of gastroenterologist physician visits, more hospitalizations, and greater rates of ED visits in rural IBD patients. These disparities in health services use result in costlier care for rural patients. Innovative methods of delivering gastroenterology care to rural IBD patients (such as telehealth, online support, and remote clinics) should be explored, especially for communities lacking easy access to gastroenterologists.
Keywords: access to care; epidemiology; health administrative data; health services research; inflammatory bowel disease; routinely collected health data.
Conflict of interest statement
Disclosure Eric I Benchimol and Geoffrey C Nguyen were supported by New Investigator Awards from CIHR, Crohn’s and Colitis Canada, and the Canadian Association of Gastroenterology. Eric I Benchimol was also supported by the Career Enhancement Program from the Canadian Child Health Clinician Scientist Program. M Ellen Kuenzig was supported by a Post-Doctoral Fellowship Award from CIHR, Crohn’s and Colitis Canada, and the Canadian Association of Gastroenterology. Charles N Bernstein was supported in part by the Bingham Chair in Gastroenterology. Geoffrey C Nguyen and Gilaad G Kaplan were CIHR Embedded Clinician Research Chairs. Astrid Guttmann was supported by a CIHR Applied Chair in Reproductive and Child Health Services and Policy Research. Lisa M Lix was supported by a Canada Research Chair (Tier I). The authors report no other conflicts of interest in this work.
Figures
References
-
- Justice Laws Website [webpage on the Internet] Canada Health Act. R.S.C., 1985c. C-6; 1985. [AccessedJuly 8, 2017]. Available from: http://laws-lois.justice.gc.ca/eng/acts/C-6/
-
- Benchimol EI, To T, Griffiths AM, Rabeneck L, Guttmann A. Outcomes of pediatric inflammatory bowel disease: socioeconomic status disparity in a universal-access healthcare system. J Pediatr. 2011;158(6):60, 967.e1–4. - PubMed
-
- Benchimol E, Boualit M, Wong J, Colombel J-F, Gower-Rousseau C. Predictors of the need for second intestinal resection in children with Crohn’s disease. Inflamm Bowel Dis. 2011;17:S6.
-
- Chassin MR, Galvin RW. The urgent need to improve health care quality. Institute of Medicine National Roundtable on Health Care Quality. JAMA. 1998;280(11):1000–1005. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
