

Gross tumour delineation on computed tomography and positron emission tomography-computed tomography in oesophageal cancer: A nationwide study
- PMID: 30519647
- PMCID: PMC6260422
- DOI: 10.1016/j.ctro.2018.10.003
Gross tumour delineation on computed tomography and positron emission tomography-computed tomography in oesophageal cancer: A nationwide study
Abstract
Background and purpose: Accurate delineation of the primary tumour is vital to the success of radiotherapy and even more important for successful boost strategies, aiming for improved local control in oesophageal cancer patients. Therefore, the aim was to assess delineation variability of the gross tumour volume (GTV) between CT and combined PET-CT in oesophageal cancer patients in a multi-institutional study.
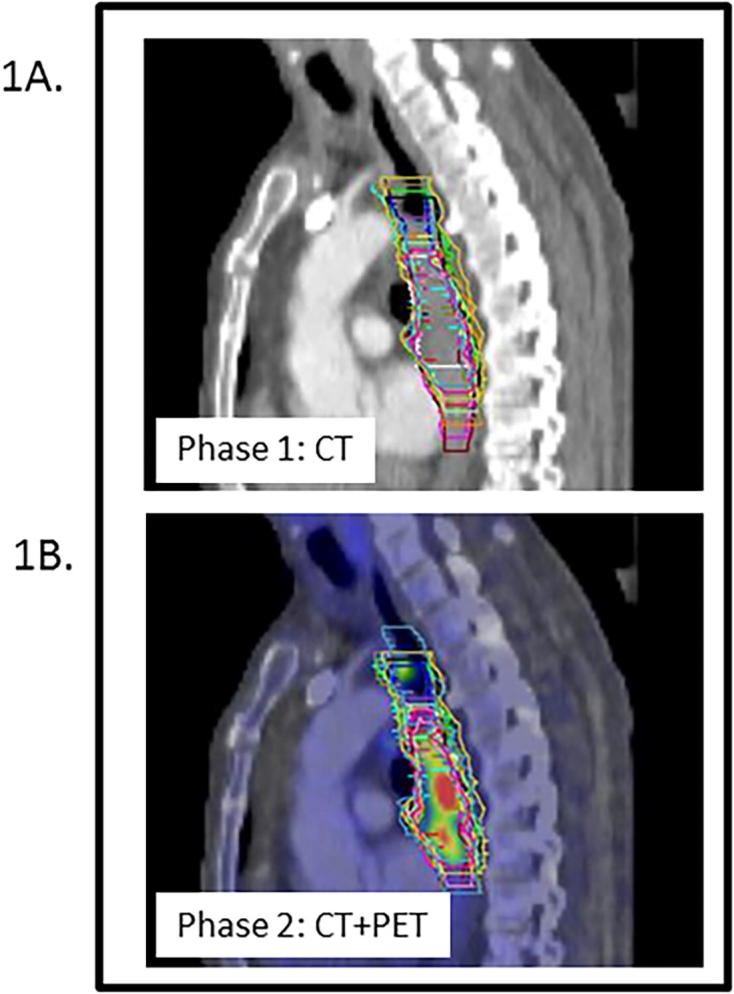
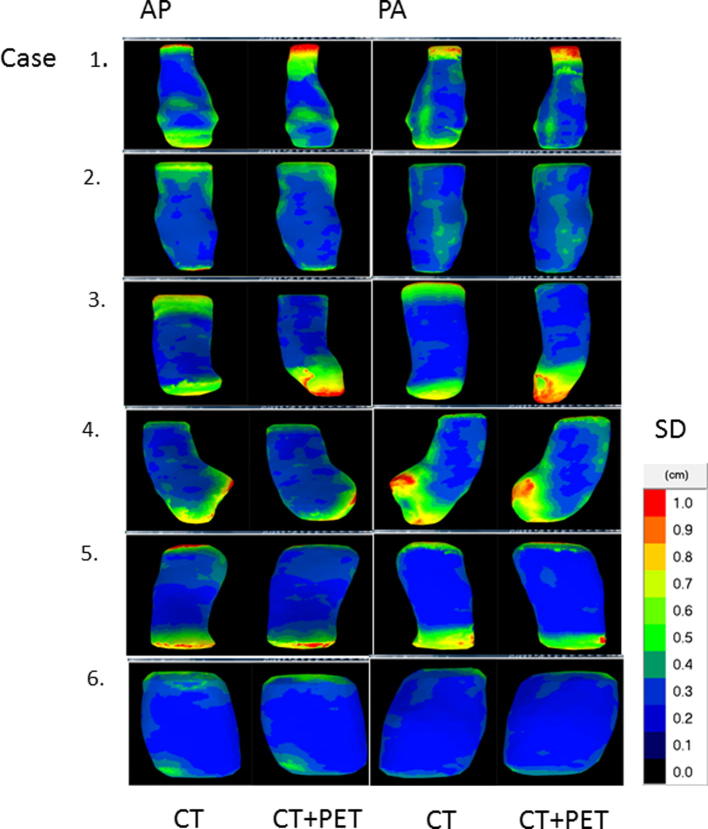
Materials and methods: Twenty observers from 14 institutes delineated the primary tumour of 6 cases on CT and PET-CT fusion. The delineated volumes, generalized conformity index (CIgen) and standard deviation (SD) in position of the most cranial/caudal slice over the observers were evaluated. For the central delineated region, perpendicular distance between median surface GTV and each individual GTV was evaluated as in-slice SD.
Results: After addition of PET, mean GTVs were significantly smaller in 3 cases and larger in 1 case. No difference in CIgen was observed (average 0.67 on CT, 0.69 on PET-CT). On CT cranial-caudal delineation variation ranged between 0.2 and 1.5 cm SD versus 0.2 and 1.3 cm SD on PET-CT. After addition of PET, the cranial and caudal variation was significantly reduced in 1 and 2 cases, respectively. The in-slice SD was on average 0.16 cm in both phases.
Conclusion: In some cases considerable GTV delineation variability was observed at the cranial-caudal border. PET significantly influenced the delineated volume in four out of six cases, however its impact on observer variation was limited.
Keywords: AJCC, American Joint Committee on Cancer; CIgen, generalized conformity index; Chemoradiotherapy; EGJ, oesophageal-gastric junction; FDG-PET/CT; GTV delineation; GTV, gross tumour volume; Interobserver variability; Oesophageal cancer; SD, standard deviation; SUV, standardized uptake volume; dCRT, definitive chemoradiation; nCR, neoadjuvant chemoradiation.
Figures
References
-
- Ferlay J., Steliarova-Foucher E., Lortet-Tieulent J., Rosso S., Coebergh J.W., Comber H. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49:1374–1403. - PubMed
-
- Shapiro J., van Lanschot J.J.B., Hulshof M., van Hagen P., van Berge Henegouwen M.I., Wijnhoven B.P.L. Neoadjuvant chemoradiotherapy plus surgery versus surgery alone for oesophageal or junctional cancer (CROSS): long-term results of a randomised controlled trial. Lancet Oncol. 2015;16:1090–1098. - PubMed
-
- Sjoquist K.M., Burmeister B.H., Smithers B.M., Zalcberg J.R., Simes R.J., Barbour A. Survival after neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal carcinoma: an updated meta-analysis. Lancet Oncol. 2011;12:681–692. - PubMed
-
- Amini A., Ajani J., Komaki R., Allen P.K., Minsky B.D., Blum M. Factors associated with local-regional failure after definitive chemoradiation for locally advanced esophageal cancer. Ann Surg Oncol. 2014;21:306–314. - PubMed
-
- Bedenne L., Michel P., Bouche O., Milan C., Mariette C., Conroy T. Chemoradiation followed by surgery compared with chemoradiation alone in squamous cancer of the esophagus: FFCD 9102. J Clin Oncol. 2007;25:1160–1168. - PubMed
LinkOut - more resources
Full Text Sources
