

Colo-Pro: a pilot randomised controlled trial to compare standard bolus-dosed cefuroxime prophylaxis to bolus-continuous infusion-dosed cefuroxime prophylaxis for the prevention of infections after colorectal surgery
- PMID: 30519893
- PMCID: PMC6514115
- DOI: 10.1007/s10096-018-3435-z
Colo-Pro: a pilot randomised controlled trial to compare standard bolus-dosed cefuroxime prophylaxis to bolus-continuous infusion-dosed cefuroxime prophylaxis for the prevention of infections after colorectal surgery
Abstract
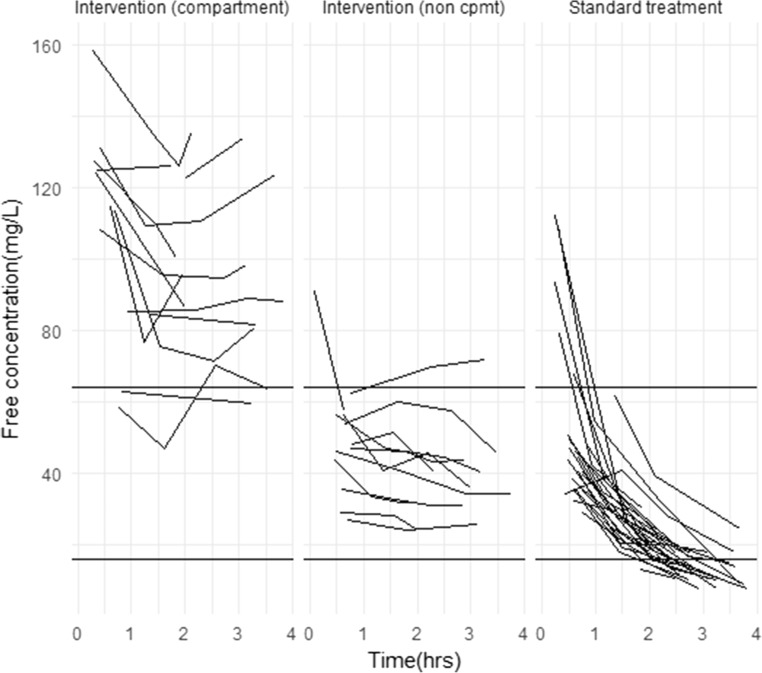
Standard bolus-dosed antibiotic prophylaxis may not inhibit growth of antibiotic resistant colonic bacteria, a cause of SSIs after colorectal surgery. An alternative strategy is continuous administration of antibiotic throughout surgery, maintaining concentrations of antibiotics that inhibit growth of resistant bacteria. This study is a pilot comparing bolus-continuous infusion with bolus-dosed cefuroxime prophylaxis in colorectal surgery. This is a pilot randomised controlled trial in which participants received cefuroxime bolus-infusion (intervention arm) targeting free serum cefuroxime concentrations of 64 mg/L, or 1.5 g cefuroxime as a bolus dose four-hourly (standard arm). Patients in both arms received metronidazole (500 mg intravenously). Eligible participants were adults undergoing colorectal surgery expected to last for over 2 h. Results were analysed on an intention-to-treat basis. The study was successfully piloted, with 46% (90/196) of eligible patients recruited and 89% (80/90) of participants completing all components of the protocol. A trialled bolus-continuous dosing regimen was successful in maintaining free serum cefuroxime concentrations of 64 mg/L. No serious adverse reactions were identified. Rates of SSIs (superficial and deep SSIs) were lower in the intervention arm than the standard treatment arm (24% (10/42) vs. 30% (13/43)), as were infection within 30 days of operation (41% (17/43) vs 51% (22/43)) and urinary tract infections (2% (1/42) vs. 9% (4/43)). These infection rates can be used to power future clinical trials. This study demonstrates the feasibility of cefuroxime bolus-continuous infusion of antibiotic prophylaxis trials, and provides safety data for infusions targeting free serum cefuroxime concentrations of 64 mg/L. Trial registration: NCT02445859 .
Keywords: Antibiotic; Bolus; Cefuroxime; Colorectal; Continuous, infusion; Prophylaxis.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures
References
-
- HES data: Health and Social Care Information Centre. Hospital Episode Statistics. http://www.hesonline.nhs.uk/Ease/servlet/ContentServer?siteID=1937. Accessed 11June 2018
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
