

Oral and intrauterine progestogens for atypical endometrial hyperplasia
- PMID: 30521671
- PMCID: PMC6517239
- DOI: 10.1002/14651858.CD009458.pub3
Oral and intrauterine progestogens for atypical endometrial hyperplasia
Abstract
Background: Endometrial carcinoma is the most common gynaecologic malignancy in the world and develops through preliminary stages of endometrial hyperplasia. Atypical endometrial hyperplasia suggests a significant pre-malignant state with frank progression to endometrial carcinoma, and tends to occur at a young age. Oral progestins have been used as conservative treatment in young women with atypical endometrial hyperplasia, but they are associated with poor tolerability and side effects that may limit their overall efficacy. So it has become increasingly important and necessary to find a safe and effective fertility-sparing treatment with better tolerability and fewer side effects than the options currently available. The levonorgestrel-releasing intrauterine system (LNG-IUS) has been used to provide endometrial protection in women with breast cancer who are on adjuvant tamoxifen. The antiproliferative function of levonorgestrel is thought to reduce the risk of endometrial hyperplasia.
Objectives: To determine the efficacy and safety of oral and intrauterine progestogens in treating atypical endometrial hyperplasia.
Search methods: In July 2018 we searched CENTRAL; MEDLINE; Embase; CINAHL, PsycINFO and the China National Knowledge Infrastructure for relevant trials. Cochrane Gynaecology and Fertility (CGF) Specialised Register and Embase were searched in November 2018. We attempted to identify trials from references in published studies. We also searched for ongoing trials in five major clinical trials registries.
Selection criteria: Randomised controlled trials (RCTs) of oral and intrauterine progestogens (LNG-IUS) versus each other or placebo in women with a confirmed histological diagnosis of simple or complex endometrial hyperplasia with atypia.
Data collection and analysis: Two review authors assessed trial eligibility and risk of bias and extracted the data. The primary outcomes of the review were rate of regression and adverse effects. Secondary outcomes included rate of recurrence and proportion of women undergoing hysterectomy. We have used GRADE methodology to judge the quality of the evidence.
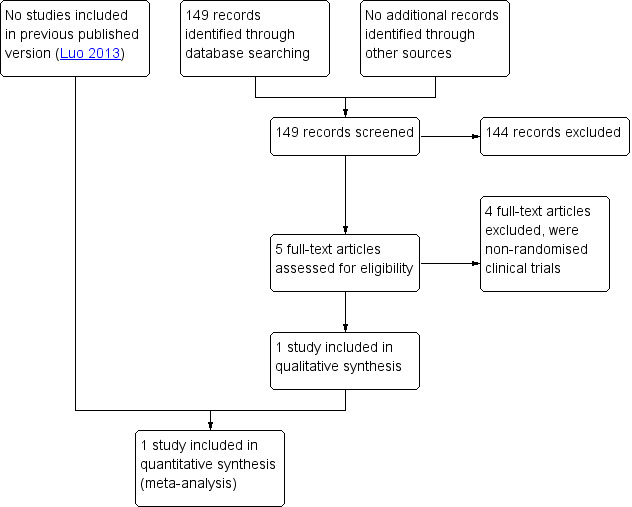
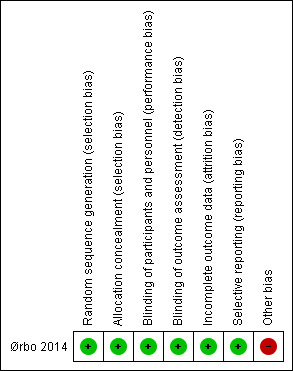
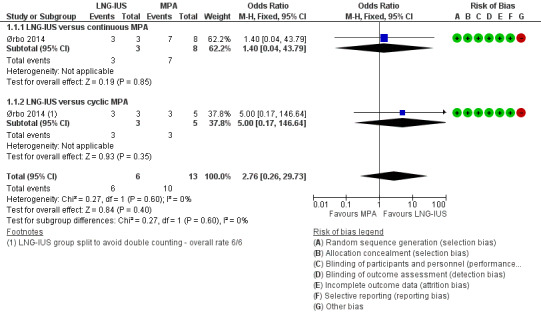
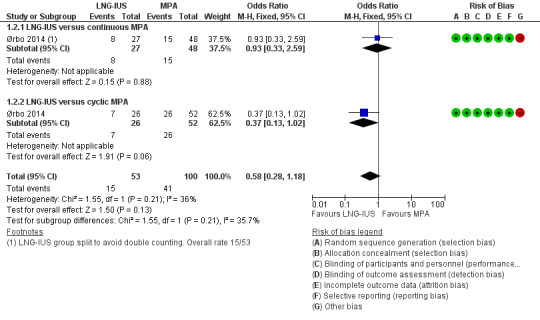
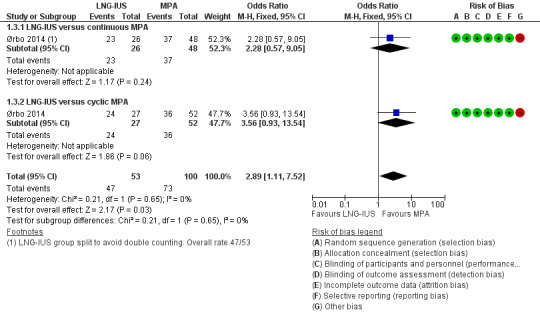
Main results: We included one RCT (153 women) comparing the LNG-IUS administering 20 micrograms (μu) levonorgestrel per day versus 10 milligrams of continuous or cyclical oral medroxyprogesterone (MPA) for treating any type of endometrial hyperplasia. Only 19 women in this study were histologically confirmed with atypical complex hyperplasia before treatment. The evidence was of low or very low quality. The included study was at low risk of bias, but the quality of the evidence was very seriously limited by imprecision and indirectness. We did not find any RCTS comparing the LNG-IUS or oral progestogens versus placebo in women with atypical endometrial hyperplasia.Among the 19 women with atypical complex hyperplasia, after six months of treatment there was insufficient evidence to determine whether there was a difference in regression rates between the LNG-IUS group and the progesterone group (odds ratio (OR) 2.76, 95% confidence interval (CI) 0.26 to 29.73; 1 RCT subgroup, 19 women, very low-quality evidence). The rate of regression was 100% in the LNG-IUS group (n = 6/6) and 77% in the progesterone group (n = 10/13).Among the total study population (N = 153), over the six months' treatment the main adverse effects were nausea and vaginal bleeding. There was no evidence of a difference between the groups in rates of nausea (OR 0.58, 95% CI 0.28 to 1.18; 1 RCT, 153 women, very low-quality evidence). Vaginal bleeding was more common in the LNG-IUS group (OR 2.89, 95% CI 1.11 to 7.52; 1 RCT, 153 women, low-quality evidence). Except for nausea and vaginal bleeding, no other adverse effects were reported.
Authors' conclusions: We did not find any RCTS of women with atypical endometrial hyperplasia, and our findings derive from a subgroup of 19 women in a larger RCT. All six women who used the LNG-IUS system achieved regression of atypical hyperplasia, but there was insufficient evidence to draw any conclusions regarding the relative efficacy of LNG-IUS versus oral progesterone (MPA) in this group of women. When assessed in a population of women with any type of endometrial hyperplasia, there was no clear evidence of a difference between LNG-IUS and oral progesterone (MPA) in risk of nausea, but vaginal bleeding was more likely to occur in women using the LNG-IUS. Larger studies are necessary to assess the efficacy and safety of oral and intrauterine progestogens in treating atypical endometrial hyperplasia.
Conflict of interest statement
Li Jing, Luo Bing, Luo Li, Neil Sidell, Zhang Heng and Zheng Ying have no interests to declare.
Figures



Update of
-
Levonorgestrel-releasing intrauterine system for atypical endometrial hyperplasia.Cochrane Database Syst Rev. 2013 Jun 5;(6):CD009458. doi: 10.1002/14651858.CD009458.pub2. Cochrane Database Syst Rev. 2013. Update in: Cochrane Database Syst Rev. 2018 Dec 04;12:CD009458. doi: 10.1002/14651858.CD009458.pub3. PMID: 23737032 Updated.
References
References to studies included in this review
References to studies excluded from this review
Buttini 2009 {published data only}
-
- Buttini MJ, Jordan SJ, Webb PM. The effect of the levonorgestrel releasing intrauterine system on endometrial hyperplasia: an Australian study and systematic review. The Australian & New Zealand Journal of Obstetrics & Gynaecology 2009;49(3):316‐22. - PubMed
Lee 2010 {published data only}
Pronin 2015 {published data only}
-
- Pronin SM, Novikova OV, Andreeva JY, Novikova EG. Fertility‐sparing treatment of early endometrial cancer and complex atypical hyperplasia in young women of childbearing potential. International Journal of Gynecological Cancer 2015;25(6):1010‐14. - PubMed
Vilos 2011 {published data only}
-
- Vilos GA, Marks J, Tureanu V, Abu‐Rafea B, Vilos AG. The levonorgestrel intrauterine system is an effective treatment in selected obese women with abnormal uterine bleeding. Journal of Minimally Invasive Gynecology 2011;18(1):75‐80. - PubMed
Additional references
Chi 1994
-
- Chi IC, Farr G. The non‐contraceptive of the levonorgestrel‐releasing intrauterine device. Advances in Contraception 1994;10(4):271‐85. - PubMed
Cozza 2017
-
- Cozza G, Pinto A, Giovanaie V, Bianchi P, Guarino A, Marziani R, et al. Comparative effective and impact on health‐related quality of life of hysterectomy vs. levonorgestrel intra‐uterine system for abnormal uterine bleeding. Eur Rev Med Pharmacol Sci 2017;21(9):2255‐2260. - PubMed
Critchley 2007
-
- Guttinger A, Critchley HO. Endometrial effects of intrauterine levonorgestrel. Contraception 2007;75(6 Suppl):93‐8. - PubMed
Dominick 2015
Eralil 2016
GRADEpro GDT 2015 [Computer program]
-
- GRADE Working Group, McMaster University. GRADEpro GDT. Version accessed 26 July 2017. Hamilton (ON): GRADE Working Group, McMaster University, 2015. Available at gradepro.org.
Guo 1993
-
- Guo LN. Atypical hyperplasia and complex hyperplasia of endometrium in women of reproductive age. Zhonghua Fu Chan Ke Za Zhi 1993;28(12):725‐7, 760. - PubMed
Higgins 2002
-
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21:1539‐58. - PubMed
Higgins 2003
Higgins 2011
-
- Higgins JP, Green S, editor(s). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from handbook.cochrane.org.
Kullander 1992
-
- Kullander S. Treatment of endometrial cancer with GnRH analogs. Recent Results in Cancer Research 1992;124:69‐73. - PubMed
Kurman 1985
-
- Kurman RJ, Kaminski PF, Norris HJ. The behavior of endometrial hyperplasia. A long‐term study of "untreated" hyperplasia in 170 patients. Cancer 1985;56(2):403‐12. - PubMed
Luukkainen 1991
-
- Luukkainen T. Levonorgestrel‐releasing intrauterine device. Annals of the New York Academy of Sciences 1991;626:43‐9. - PubMed
Qi 2008
-
- Qi X, Zhao W, Duan Y, Li Y. Successful pregnancy following insertion of a levonorgestrel‐releasing intrauterine system in two infertile patients with complex atypical endometrial hyperplasia. Gynecologic and Obstetric Investigation 2008;65(4):266‐8. - PubMed
Randall 1997
-
- Randall TC, Kurman RJ. Progestin treatment of atypical hyperplasia and well‐differentiated carcinoma of the endometrium in women under age 40. Obstetrics and Gynecology 1997;90(3):434‐40. - PubMed
RevMan 2014 [Computer program]
-
- Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager 5 (RevMan 5). Version 5.3. Copenhagen: Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Sitruk‐Ware 2004
-
- Sitruk‐Ware R. Pharmacological profile of progestins. Maturitas 2004;47(4):277‐83. - PubMed
Sturridge 1996
-
- Sturridge F, Guillebaud J. A risk‐benefit assessment of the levonorgestrel‐releasing intrauterine system. Drug Safety 1996;15(6):430‐40. - PubMed
Wildemeersch 2003
-
- Wildemeersch D, Dhont M. Treatment of non‐atypical and atypical endometrial hyperplasia with a levonorgestrel‐releasing intrauterine system. American Journal of Obstetrics and Gynecology 2003;188(5):1297‐8. - PubMed
Wildemeersch 2007
-
- Wildemeersch D, Janssens D, Pylyser K, Wever DE, Verbeeck G, Dhont M, et al. Management of patients with non‐atypical and atypical endometrial hyperplasia with a levonorgestrel‐releasing intrauterine system: long‐term follow‐up. Maturitas 2007;57(2):210‐3. - PubMed
Xiao 1990
-
- Xiao BL, Zhou LY, Zhang XL, Jia MC, Luukkainen T, Allonen H. Pharmacokinetic and pharmacodynamic studies of levonorgestrel‐releasing intrauterine device. Contraception 1990;41(4):353‐62. - PubMed
References to other published versions of this review
Luo 2011
-
- Luo L, Luo B, Zheng Y, Zhang H, Li J, Sidell N. Levonorgestrel‐releasing intrauterine system for atypical endometrial hyperplasia. Cochrane Database of Systematic Reviews 2011, Issue 11. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources