

National survey: current prevalence and characteristics of home mechanical ventilation in Hungary
- PMID: 30522473
- PMCID: PMC6282340
- DOI: 10.1186/s12890-018-0754-x
National survey: current prevalence and characteristics of home mechanical ventilation in Hungary
Abstract
Background: Home mechanical ventilation is an established treatment for chronic respiratory failure resulting in improved survival and quality of life. Technological advancement, evolving health care reimbursement systems and newly implemented national guidelines result in increased utilization worldwide. Prevalence shows great geographical variations and data on East-Central European practice has been scarce to date. The aim of the current study was to evaluate prevalence and characteristics of home mechanical ventilation in Hungary.
Methods: We conducted a nationwide study using an online survey focusing on patients receiving ventilatory support at home. The survey focused on characterization of the site (affiliation, type), experience with home mechanical ventilation, number of patients treated, indication for home mechanical ventilation (disease type), description of home mechanical ventilation (invasive/noninvasive, ventilation hours, duration of ventilation) and description of the care provided (type of follow up visits, hospitalization need, reimbursement).
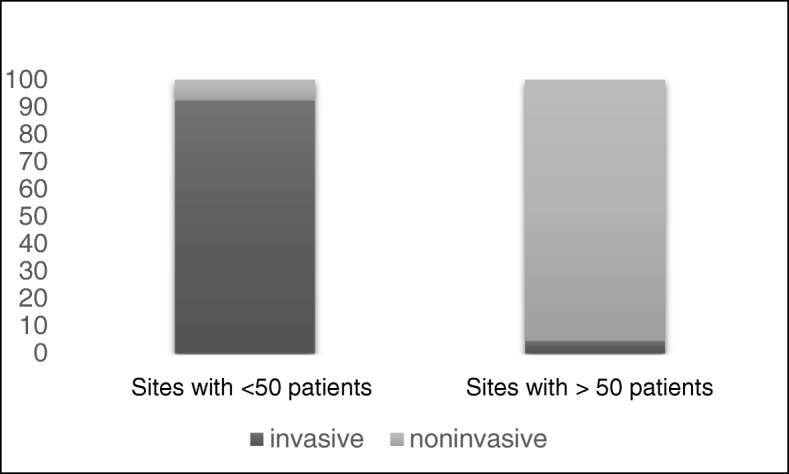
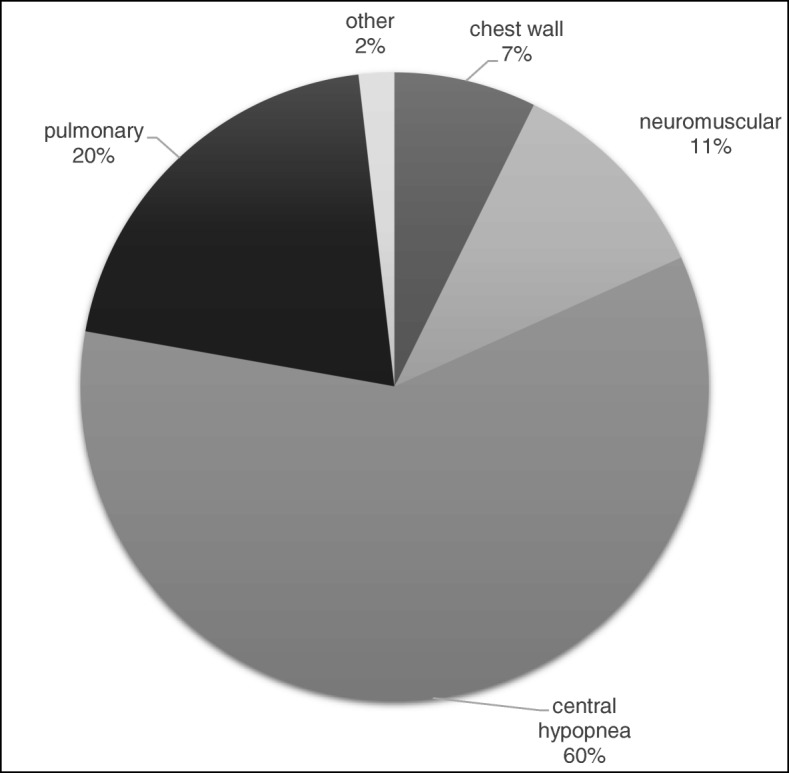
Results: Our survey uncovered a total of 384 patients amounting to a prevalence of 3.9/100,000 in Hungary. 10.4% of patients received invasive, while 89.6% received noninvasive ventilation. The most frequent diagnosis was central hypopnea syndromes (60%), while pulmonary (20%), neuromuscular (11%) and chest wall disorders (7%) were less frequent indications. Daily ventilation need was less than 8 h in 74.2%, between 8 and 16 h in 15.4% and more than 16 h in 10.4% of patients reported. When comparing sites with a limited (< 50 patients) versus substantial (> 50 patients) case number, we found the former had significantly higher ratio of neuromuscular conditions, were more likely to ventilate invasively, with more than 16 h/day ventilation need and were more likely to provide home visits and readmit patients (p < 0,001).
Conclusions: Our results show a reasonable current estimate and characterization of home mechanical ventilation practice in Hungary. Although a growing practice can be assumed, current prevalence is still markedly reduced compared to international data reported, the duality of current data hinting to a possible gap in diagnosis and care for more dependent patients. This points to the importance of establishing home mechanical ventilation centers, where increased experience will enable state of the art care to more dependent patients as well, increasing overall prevalence.
Keywords: Chronic respiratory failure; Home care; Home mechanical ventilation.
Conflict of interest statement
Authors’ information
JG is the head of the Department of Anesthesiology and Intensive Therapy at Semmelweis University, overseeing the Semmelweis University Home Mechanical Ventilation Program, headed by AL. LV and SB have been involved with the Program since its establishment in 2014.
Ethics approval and consent to participate
The study was approved by the research ethics board of Semmelweis University (SE TUKEB 253/2017). Participation was voluntary and consent was implied by response to the survey.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- van den Bergen JC, Ginjaar HB, van Essen AJ, Pangalila R, de Groot IJ, Wijkstra PJ, et al. Forty-five years of Duchenne muscular dystrophy in the Netherlands. J Neuromusc Dis. 2014;1:99–109. - PubMed
-
- Kohnlein T, Windisch W, Kohler D, Drabik A, Geiseler J, Hartl S, et al. Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial. Lancet Respir Med. 2014;2:698–705. doi: 10.1016/S2213-2600(14)70153-5. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
