

Bleeding Complications after Pediatric Kidney Biopsy: A Systematic Review and Meta-Analysis
- PMID: 30522995
- PMCID: PMC6364534
- DOI: 10.2215/CJN.05890518
Bleeding Complications after Pediatric Kidney Biopsy: A Systematic Review and Meta-Analysis
Abstract
Background and objectives: Kidney biopsy is an essential tool for the diagnosis and treatment of patients with kidney disease; however, because of its invasive nature, bleeding complications may arise.
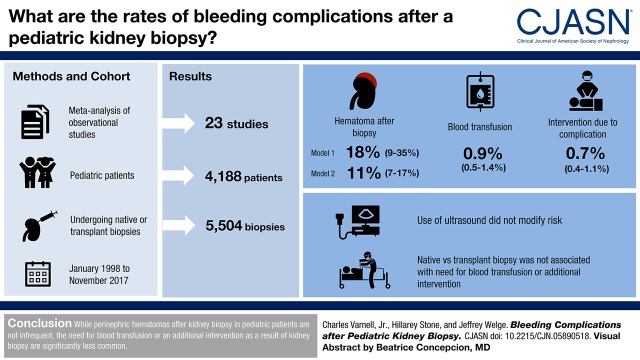
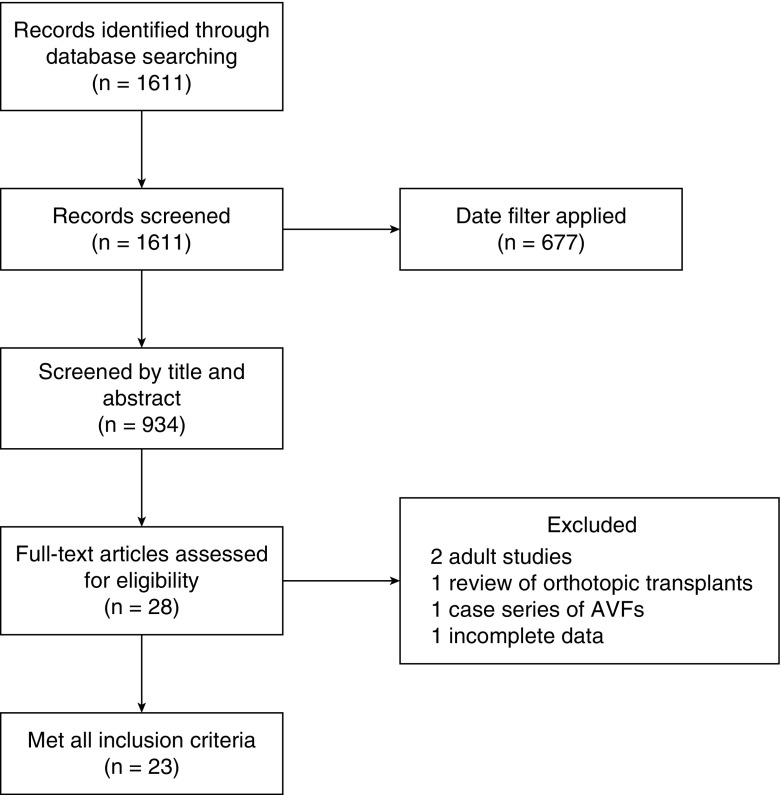
Design, setting, participants, & measurements: We performed a meta-analysis of prospective or retrospective observational studies and randomized, controlled trials in pediatric patients undergoing native or transplant kidney biopsy in an inpatient or outpatient setting in MEDLINE-indexed studies from January 1998 to November 1, 2017 to determine the proportion of patients who develop hematoma, need blood transfusion, or need an additional intervention due to a complication after kidney biopsy.
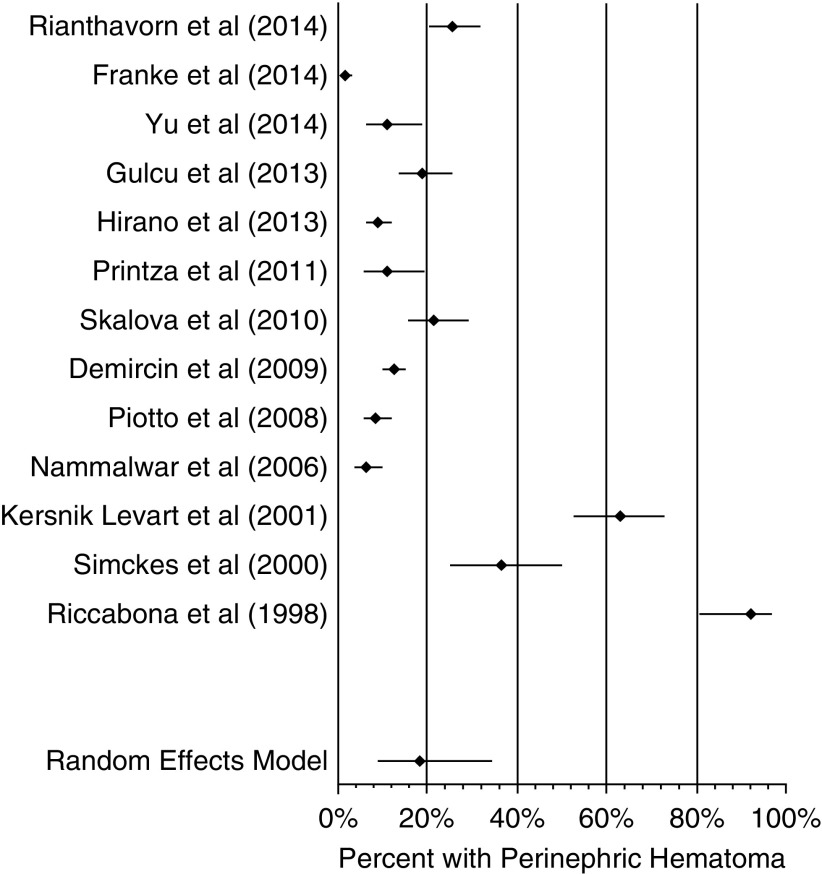
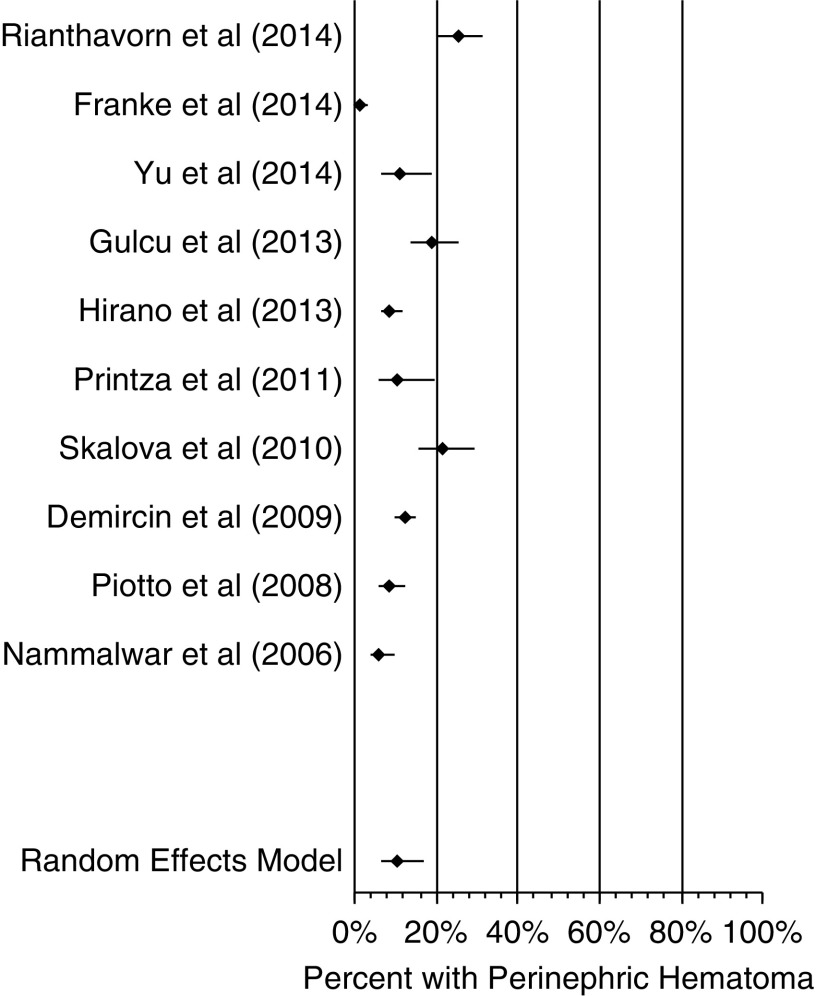
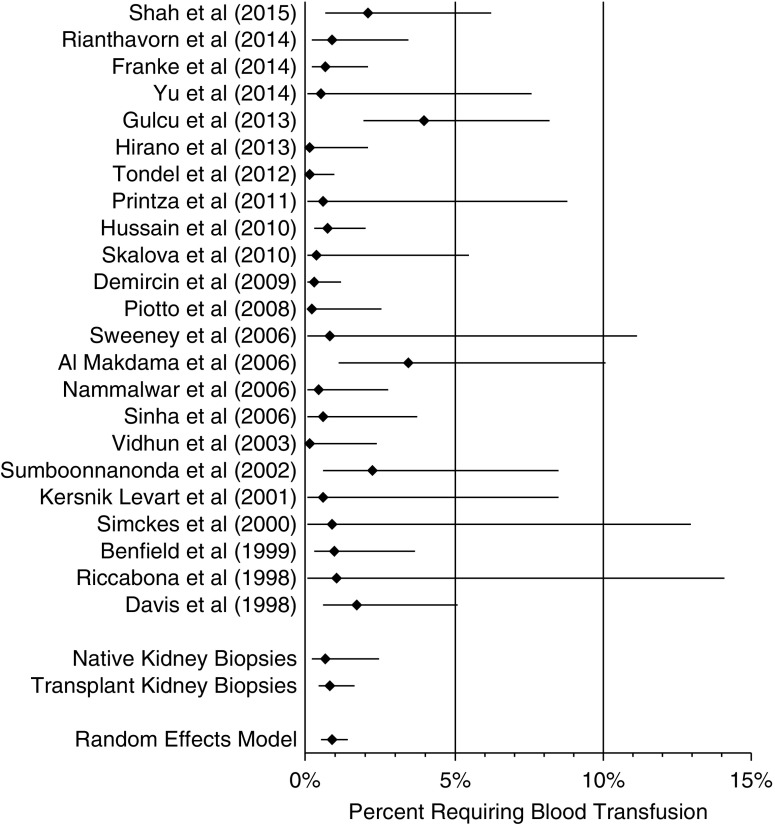
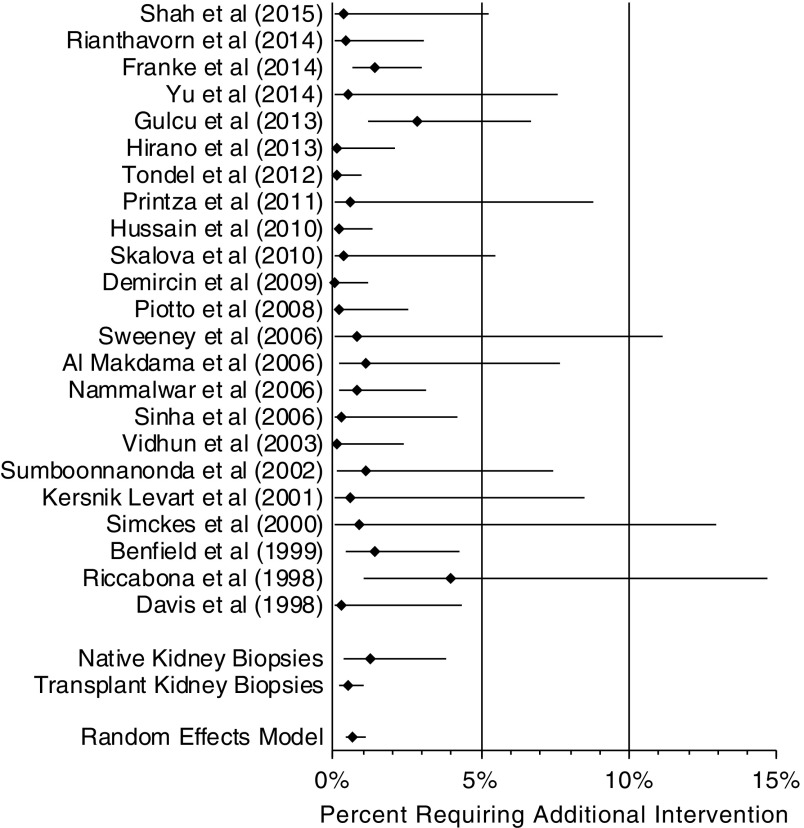
Results: Twenty-three studies of 5504 biopsies met inclusion criteria. The proportion of patients developing hematoma after biopsy was between 11% (95% confidence interval, 7% to 17%) and 18% (95% confidence interval, 9% to 35%) using two analyses that included different time periods. The proportion needing blood transfusion was 0.9% (95% confidence interval, 0.5% to 1.4%). The proportion needing an additional intervention due to postbiopsy complication was 0.7% (95% confidence interval, 0.4% to 1.1%). Secondary analysis was not possible due to lack of data in the original manuscripts on laboratory values, needle gauges, number of needle passes, age of patient, or performer (attending versus trainee). Analysis with metaregression found that use of real-time ultrasound during biopsy did not modify the risk for hematoma, requirement of a blood products transfusion, or requirement of an additional procedure after biopsy. Analysis with metaregression comparing native biopsies with transplant biopsies did not reveal that biopsy type (native kidney biopsy versus transplant kidney biopsy) was associated with the need for a blood transfusion or requirement of an additional intervention after biopsy.
Conclusions: The development of perinephric hematoma after kidney biopsy is not an infrequent finding. The proportion of patients requiring blood transfusion or needing an additional intervention as a result of kidney biopsy in pediatric patients is significantly smaller.
Keywords: Biopsy; Blood Transfusion; Hematoma; Inpatients; Kidney Diseases; MEDLINE; Outpatients; Prospective Studies; Retrospective Studies; children; kidney biopsy; kidney transplantation; pediatric nephrology; renal biopsy.
Copyright © 2019 by the American Society of Nephrology.
Figures
References
-
- Avner ED, Harmon WE, Niaudet P, Yoshikawa N, Emma F, Goldstein SL: Pediatric Nephrology, 7th Ed., Berlin, Springer, 2016
-
- Clark O, Djulbegovic B: Forest Plots in Excel Software (Data Sheet), 2001. Available at www.evidencias.com. Accessed August 1, 2014
-
- Skalova S, Rejtar P: Safety profile of paediatric percutaneous ultrasonography-guided renal biopsies. Singapore Med J 51: 481–483, 2010 - PubMed
-
- Nammalwar BR, Vijayakumar M, Prahlad N: Experience of renal biopsy in children with nephrotic syndrome. Pediatr Nephrol 21: 286–288, 2006 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
