

The diagnostic accuracy of 18F-FDG PET/CT in diagnosing fracture-related infections
- PMID: 30523391
- PMCID: PMC6450834
- DOI: 10.1007/s00259-018-4218-6
The diagnostic accuracy of 18F-FDG PET/CT in diagnosing fracture-related infections
Abstract
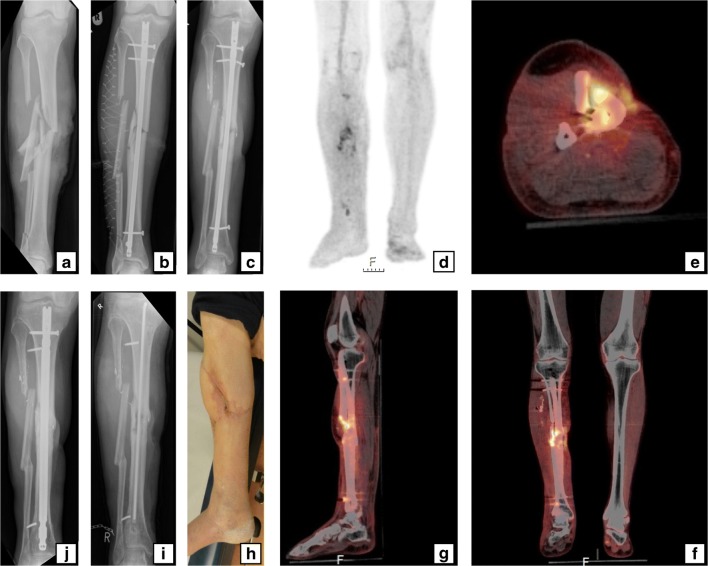
Purpose: 18F-Fluorodeoxyglucose positron emission tomography (18F-FDG PET/CT) is frequently used to diagnose fracture-related infections (FRIs), but its diagnostic performance in this field is still unknown. The aims of this study were: (1) to assess the diagnostic performance of qualitative assessment of 18F-FDG PET/CT scans in diagnosing FRI, (2) to establish the diagnostic performance of standardized uptake values (SUVs) extracted from 18F-FDG PET/CT scans and to determine their associated optimal cut-off values, and (3) to identify variables that predict a false-positive (FP) or false-negative (FN) 18F-FDG PET/CT result.
Methods: This retrospective cohort study included all patients with suspected FRI undergoing 18F-FDG PET/CT between 2011 and 2017 in two level-1 trauma centres. Two nuclear medicine physicians independently reassessed all 18F-FDG PET/CT scans. The reference standard consisted of the result of at least two deep, representative microbiological cultures or the presence/absence of clinical confirmatory signs of FRI (AO/EBJIS consensus definition) during a follow-up of at least 6 months. Diagnostic performance in terms of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) was calculated. Additionally, SUVs were measured on 18F-FDG PET/CT scans. Volumes of interest were drawn around the suspected and corresponding contralateral areas to obtain absolute values and ratios between suspected and contralateral areas. A multivariable logistic regression analysis was also performed to identify the most important predictor(s) of FP or FN 18F-FDG PET/CT results.
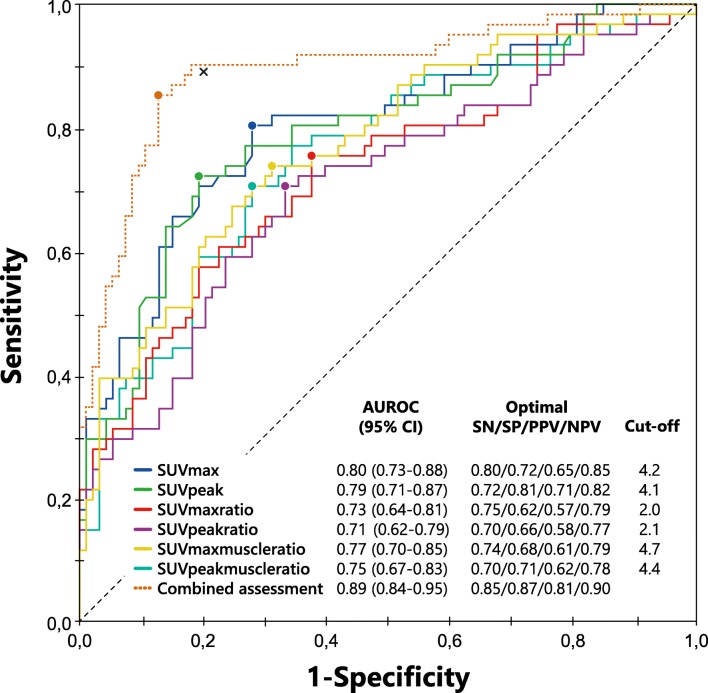
Results: The study included 156 18F-FDG PET/CT scans in 135 patients. Qualitative assessment of 18F-FDG PET/CT scans showed a sensitivity of 0.89, specificity of 0.80, PPV of 0.74, NPV of 0.91 and diagnostic accuracy of 0.83. SUVs on their own resulted in lower diagnostic performance, but combining them with qualitative assessments yielded an AUC of 0.89 compared to an AUC of 0.84 when considering only the qualitative assessment results (p = 0.007). 18F-FDG PET/CT performed <1 month after surgery was found to be the independent variable with the highest predictive value for a false test result, with an absolute risk of 46% (95% CI 27-66%), compared with 7% (95% CI 4-12%) in patients with 18F-FDG PET/CT performed 1-6 months after surgery.
Conclusion: Qualitative assessment of 18F-FDG PET/CT scans had a diagnostic accuracy of 0.83 and an excellent NPV of 0.91 in diagnosing FRI. Adding SUV measurements to qualitative assessment provided additional accuracy in comparison to qualitative assessment alone. An interval between surgery and 18F-FDG PET/CT of <1 month was associated with a sharp increase in false test results.
Keywords: 18F-FDG PET/CT; Diagnosis; Diagnostic accuracy; Diagnostic performance; Fracture-related infections; Infection; Medical imaging; Nuclear imaging; Osteomyelitis; Trauma.
Conflict of interest statement
Conflicts of interest
None.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Due to the observational nature of this study the need for informed consent was waived by the Medical Ethics Review Committee (METC) of the University Medical Center Utrecht (METC 17-475).
Figures
References
-
- Whitehouse JD, Friedman ND, Kirkland KB, Richardson WJ, Sexton DJ. The impact of surgical-site infections following orthopedic surgery at a community hospital and a university hospital: adverse quality of life, excess length of stay, and extra cost. Infect Control Hosp Epidemiol. 2002;23(4):183–189. doi: 10.1086/502033. - DOI - PubMed
-
- Govaert GA, IJpma FFA, McNally M, McNally E, Reininga IH, Glaudemans AW. Accuracy of diagnostic imaging modalities for peripheral post-traumatic osteomyelitis – a systematic review of the recent literature. Eur J Nucl Med Mol Imaging. 2017;44(8):1393–1407. doi: 10.1007/s00259-017-3683-7. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
