

Association of patterns of care, prognostic factors, and use of radiotherapy-temozolomide therapy with survival in patients with newly diagnosed glioblastoma: a French national population-based study
- PMID: 30523606
- PMCID: PMC6399437
- DOI: 10.1007/s11060-018-03065-z
Association of patterns of care, prognostic factors, and use of radiotherapy-temozolomide therapy with survival in patients with newly diagnosed glioblastoma: a French national population-based study
Abstract
Background: Glioblastoma is the most frequent primary malignant brain tumor. In daily practice and at whole country level, oncological care management for glioblastoma patients is not completely known.
Objectives: To describe oncological patterns of care, prognostic factors, and survival for all patients in France with newly-diagnosed and histologically confirmed glioblastoma, and evaluate the impact of extended temozolomide use at the population level.
Methods: Nationwide population-based cohort study including all patients with newly-diagnosed and histologically confirmed glioblastoma in France in 2008 and followed until 2015.
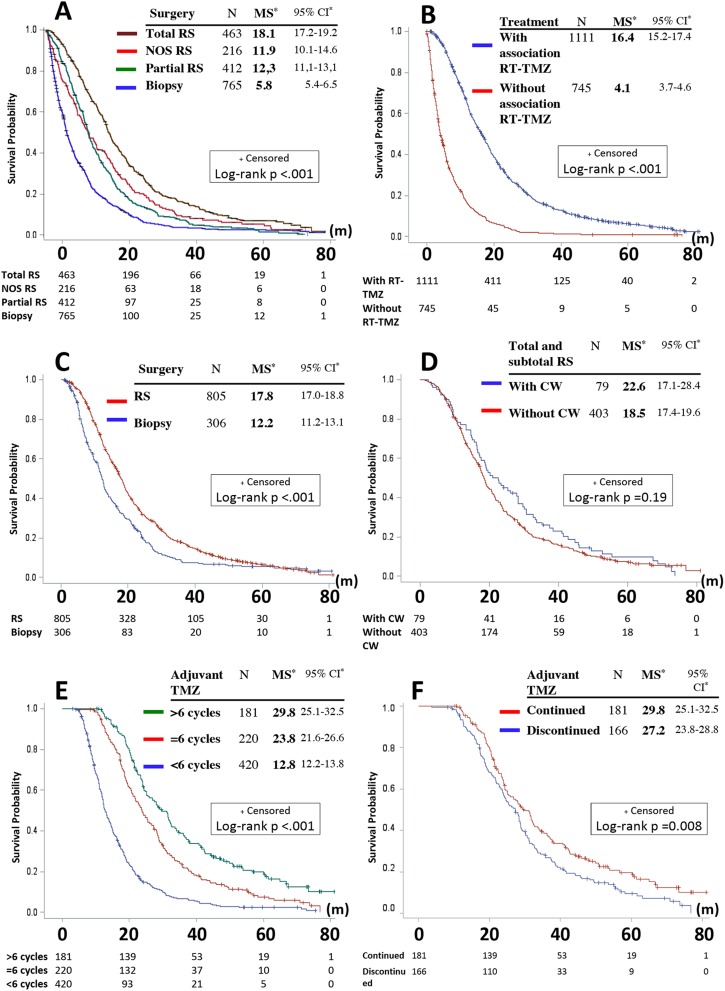
Results: Data from 2053 glioblastoma patients were analyzed (male/female ratio 1.5, median age 64 years). Median overall survival (OS) was 11.2 [95% confidence interval (CI) 10.7-11.9] months. The first-line therapy and corresponding median survival (MS, in months) were: 13% did not receive any oncological treatment (biopsy only) (MS = 1.8, 95% CI 1.6-2.1), 27% received treatment without the combination of radiotherapy (RT)-temozolomide (MS = 5.9, 95% CI 5.5-6.6), 60% received treatment including the initiation of the concomitant phase of RT-temozolomide (MS = 16.4, 95% CI 15.2-17.4) whom 44% of patients initiated the temozolomide adjuvant phase (MS = 18.9, 95% CI 18.0-19.8). Only 22% patients received 6 cycles or more of adjuvant temozolomide (MS = 25.5, 95% CI 24.0-28.3). The multivariate analysis showed that the risk of mortality was significantly higher for the non-progressive patients who stopped at 6 cycles (standard protocol) than those who continued the treatment, hazard ratio = 1.5 (95% CI 1.2-1.9).
Conclusion: In non-progressive patients, prolonging the adjuvant temozolomide beyond 6 cycles may improve OS.
Keywords: Clinical epidemiology; Glioblastoma; Neuro-oncology; Neurosurgery; Population-based study; Temozolomide.
Conflict of interest statement
None of the authors have any competing interests.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
