

Perturbation-Based Balance Training to Improve Step Quality in the Chronic Phase After Stroke: A Proof-of-Concept Study
- PMID: 30524360
- PMCID: PMC6261972
- DOI: 10.3389/fneur.2018.00980
Perturbation-Based Balance Training to Improve Step Quality in the Chronic Phase After Stroke: A Proof-of-Concept Study
Abstract
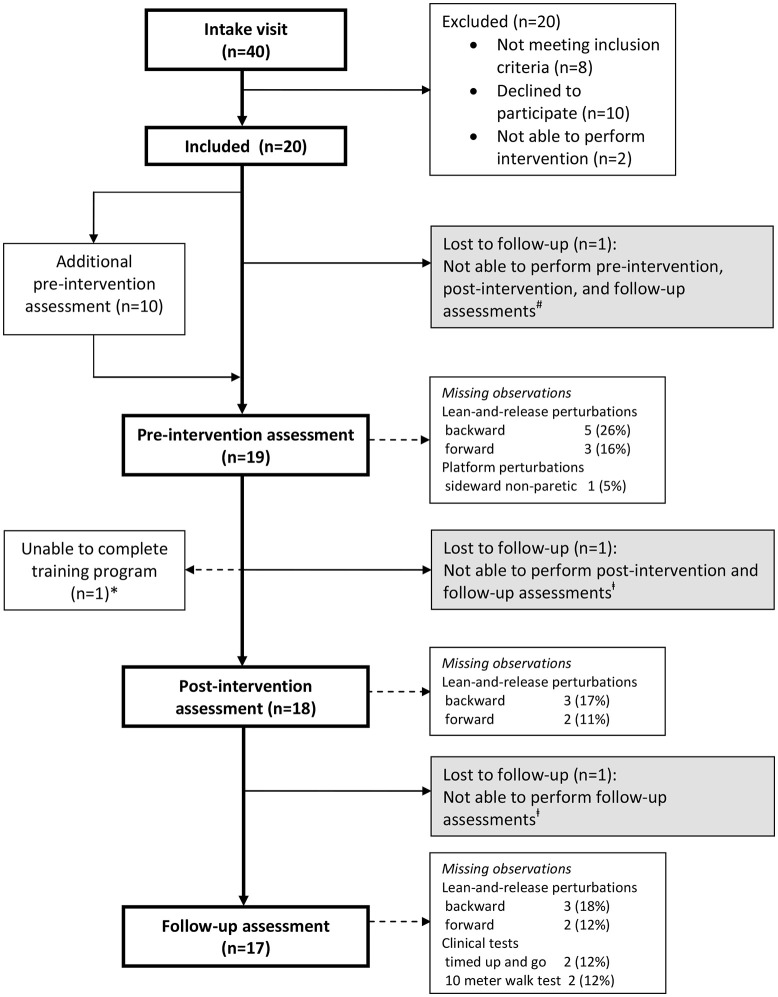
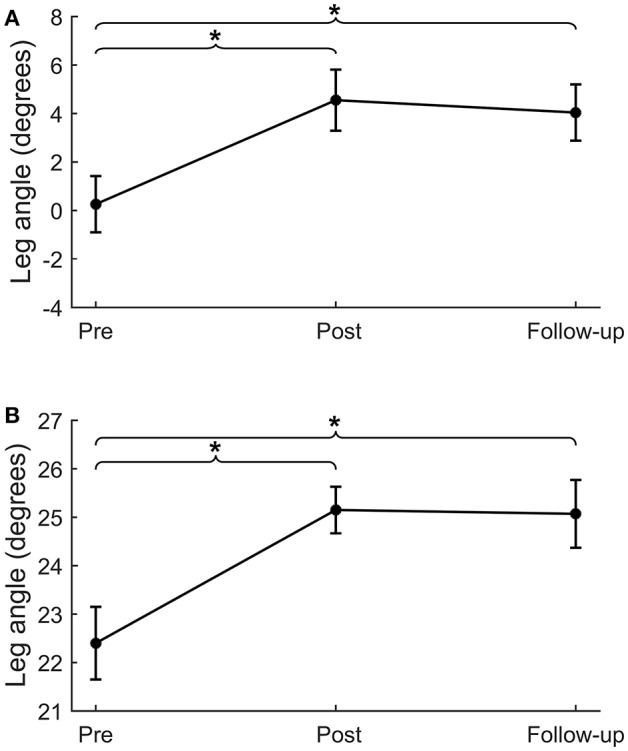
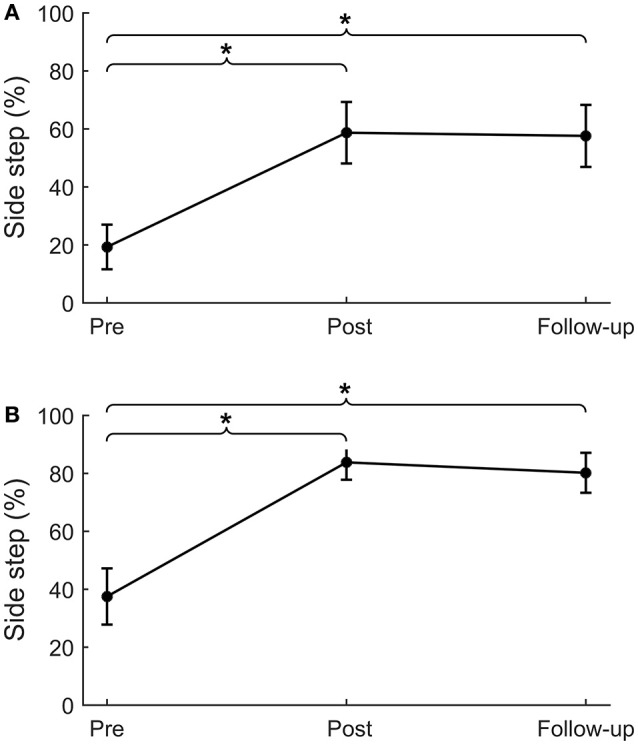
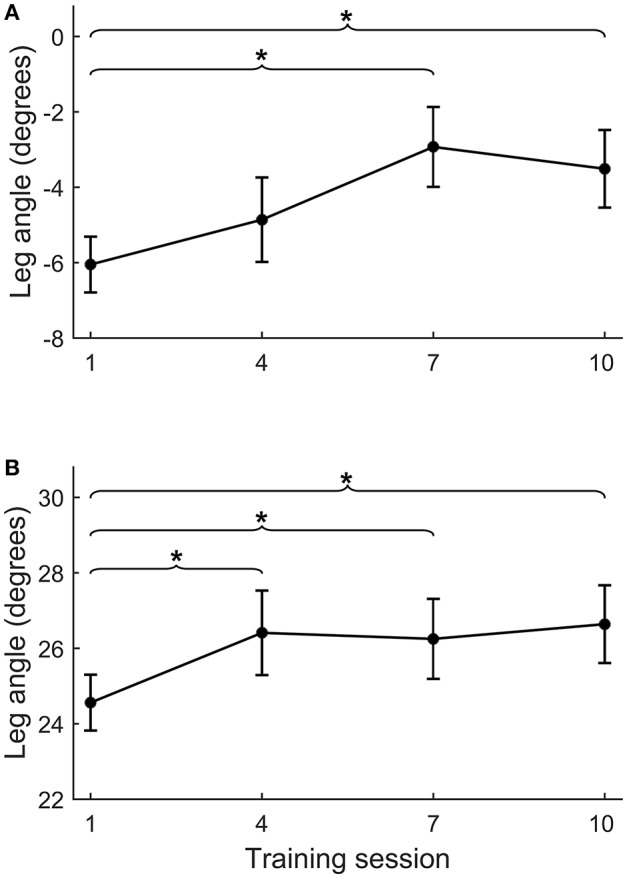
Introduction: People with stroke often have impaired stepping responses following balance perturbations, which increases their risk of falling. Computer-controlled movable platforms are promising tools for delivering perturbation-based balance training under safe and standardized circumstances. Purpose: This proof-of-concept study aimed to identify whether a 5-week perturbation-based balance training program on a movable platform improves reactive step quality in people with chronic stroke. Materials and Methods: Twenty people with chronic stroke received a 5-week perturbation-based balance training (10 sessions, 45 min) on a movable platform. As the primary outcome, backward, and forward reactive step quality (i.e., leg angle at stepping-foot contact) was assessed with a lean-and-release (i.e., non-trained) task at pre-intervention, immediately post-intervention, and 6 weeks after intervention (follow-up). Additionally, reactive step quality was assessed on the movable platform in multiple directions, as well as, the percentage side steps upon sideward perturbations. To ensure that changes in the primary outcome could not solely be attributed to learning effects on the task due to repeated testing, 10 randomly selected participants received an additional pre-intervention assessment, 6 weeks prior to training. Clinical assesments included the 6-item Activity-specific Balance Confidence (6-ABC) scale, Berg Balance Scale (BBS), Trunk Impairment Scale (TIS), 10-Meter Walking Test (10-MWT), and Timed Up and Go-test (TUG). Results: After lean-and-release, we observed 4.3° and 2.8° greater leg angles at post compared to pre-intervention in the backward and forward direction, respectively. Leg angles also significantly improved in all perturbation directions on the movable platform. In addition, participants took 39% more paretic and 46% more non-paretic side steps. These effects were retained at follow-up. Post-intervention, BBS and TIS scores had improved. At follow-up, TIS and 6-ABC scores had significantly improved compared to pre-intervention. No significant changes were observed between the two pre-intervention assessments (n=10). Conclusion: A 5-week perturbation-based balance training on a movable platform appears to improve reactive step quality in people with chronic stroke. Importantly, improvements were retained after 6 weeks. Further controlled studies in larger patient samples are needed to verify these results and to establish whether this translates to fewer falls in daily life. Trial registration: The Netherlands National Trial Register (NTR3804). http://www.trialregister.nl/trialreg/admin/rctview.aspTC=3804.
Keywords: exercise therapy; neurological rehabilitation; paresis; physical therapy modalities; postural balance.
Figures

References
LinkOut - more resources
Full Text Sources
Medical
Research Materials