

The Possible Pathophysiological Outcomes and Mechanisms of Tourniquet-Induced Ischemia-Reperfusion Injury during Total Knee Arthroplasty
- PMID: 30524661
- PMCID: PMC6247434
- DOI: 10.1155/2018/8087598
The Possible Pathophysiological Outcomes and Mechanisms of Tourniquet-Induced Ischemia-Reperfusion Injury during Total Knee Arthroplasty
Abstract
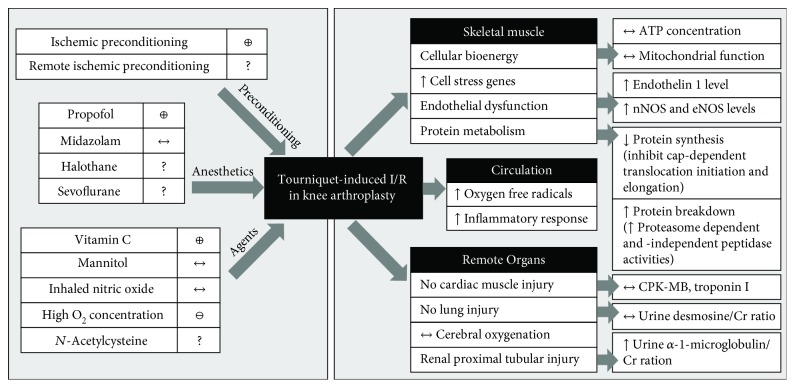
Ischemia and reperfusion (I/R) injury induced by tourniquet (TQ) application leads to the release of both oxygen free radicals and inflammatory cytokines. The skeletal muscle I/R may contribute to local skeletal muscle and remote organ damage affecting outcomes after total knee arthroplasty (TKA). The aim of the study is to summarize the current findings associated with I/R injury following TKA using a thigh TQ, which include cellular alterations and protective therapeutic interventions. The PubMed database was searched using the keywords "ischemia reperfusion injury," "oxidative stress," "tourniquet," and "knee arthroplasty." The search was limited to research articles published in the English language. Twenty-eight clinical studies were included in this qualitative review. Skeletal muscle I/R reduces protein synthesis, increases protein degradation, and upregulates genes in cell stress pathways. The I/R of the lower extremity elevates local and systemic oxidative stress as well as inflammatory reactions and impairs renal function. Propofol reduces oxidative injury in this I/R model. Ischemic preconditioning (IPC) and vitamin C may prevent oxygen free radical production. However, a high dose of N-acetylcysteine possibly induces kidney injury. In summary, TQ-related I/R during TKA leads to muscle protein metabolism alteration, endothelial dysfunction, oxidative stress, inflammatory response, and renal function disturbance. Propofol, IPC, and vitamin C show protective effects on oxidative and inflammatory markers. However, a relationship between biochemical parameters and postoperative clinical outcomes has not been validated.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
