

Lung ultrasound for the diagnosis of pneumonia in children with acute bronchiolitis
- PMID: 30526548
- PMCID: PMC6286612
- DOI: 10.1186/s12890-018-0750-1
Lung ultrasound for the diagnosis of pneumonia in children with acute bronchiolitis
Abstract
Background: Guidelines currently do not recommend the routine use of chest x-ray (CXR) in bronchiolitis. However, CXR is still performed in a high percentage of cases, mainly to diagnose or rule out pneumonia. The inappropriate use of CXR results in children exposure to ionizing radiations and increased medical costs. Lung Ultrasound (LUS) has become an emerging diagnostic tool for diagnosing pneumonia in the last decades. The purpose of this study was to assess the diagnostic accuracy and reliability of LUS for the detection of pneumonia in hospitalized children with bronchiolitis and to evaluate the agreement between LUS and CXR in diagnosing pneumonia in these patients.
Methods: We enrolled children admitted to our hospital in 2016-2017 with a diagnosis of bronchiolitis and undergone CXR because of clinical suspicion of concomitant pneumonia. LUS was performed in each child by a pediatrician blinded to the patient's clinical, laboratory and CXR findings. An exploratory analysis was done in the first 30 patients to evaluate the inter-observer agreement between a pediatrician and a radiologist who independently performed LUS. The diagnosis of pneumonia was established by an expert clinician based on the recommendations of the British Thoracic Society guidelines.
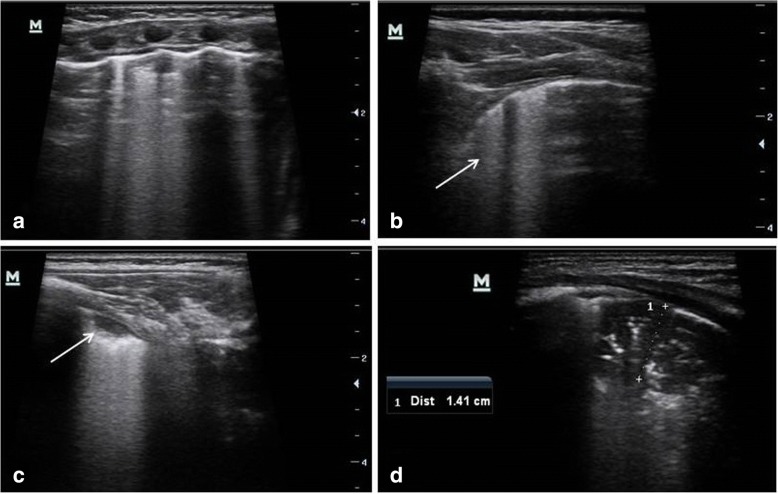
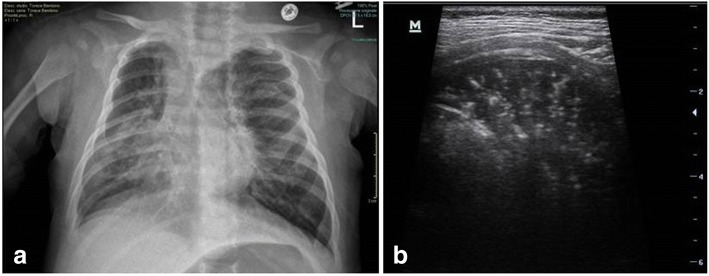
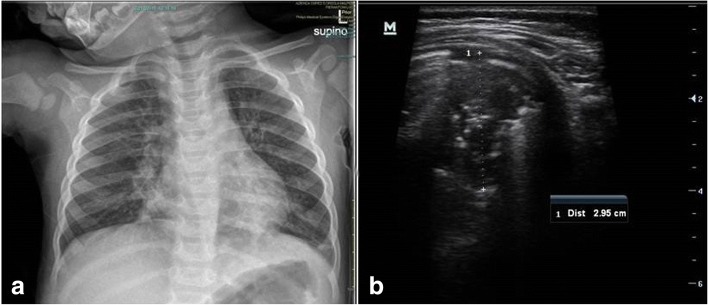
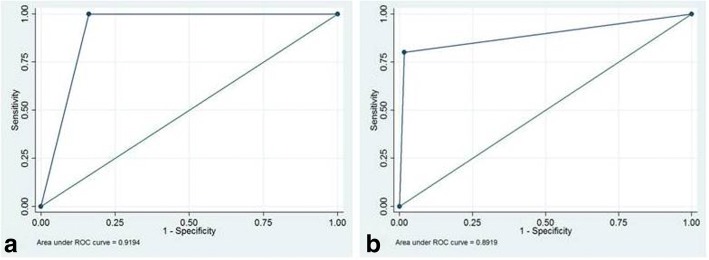
Results: Eighty seven children with bronchiolitis were investigated. A final diagnosis of concomitant pneumonia was made in 25 patients. Sensitivity and specificity of LUS for the diagnosis of pneumonia were 100% and 83.9% respectively, with an area under-the-curve of 0.92, while CXR showed a sensitivity of 96% and specificity of 87.1%. When only consolidation > 1 cm was considered consistent with pneumonia, the specificity of LUS increased to 98.4% and the sensitivity decreased to 80.0%, with an area under-the-curve of 0.89. Cohen's kappa between pediatrician and radiologist sonologists in the first 30 patients showed an almost perfect agreement in diagnosing pneumonia by LUS (K 0.93).
Conclusions: This study shows the good accuracy of LUS in diagnosing pneumonia in children with clinical bronchiolitis. When including only consolidation size > 1 cm, specificity of LUS was higher than CXR, avoiding the need to perform CXR in these patients. Added benefit of LUS included high inter-observer agreement.
Trial registration: Identifier: NCT03280732 . Registered 12 September 2017 (retrospectively registered).
Keywords: Bronchiolitis; Chest X-ray; Lung ultrasound; Pneumonia.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Institutional Ethics Committee of St. Orsola-Malpighi Hospital, University of Bologna (reference number: 13/2016/O/Sper). Parents of all the participants gave informed written consent.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Anderson EJ, Carbonell-Estrany X, Blanken M, Lanari M, Sheridan-Pereira M, Rodgers-Gray B, et al. Burden of severe respiratory syncytial virus disease among 33-35 Weeks’ gestational age infants born during multiple respiratory syncytial virus seasons. Pediatr Infect Dis J. 2017;36(2):160–167. doi: 10.1097/INF.0000000000001377. - DOI - PMC - PubMed
-
- Vandini S, Faldella G, Lanari M. Latest options for treatment of bronchiolitis in infants. Expert Rev Respir Med. 2016;9:1–9. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
