

Living at home after emergency hospital admission: prospective cohort study in older adults with and without cognitive spectrum disorder
- PMID: 30526577
- PMCID: PMC6288896
- DOI: 10.1186/s12916-018-1199-z
Living at home after emergency hospital admission: prospective cohort study in older adults with and without cognitive spectrum disorder
Abstract
Background: Cognitive spectrum disorders (CSDs) are common in hospitalised older adults and associated with adverse outcomes. Their association with the maintenance of independent living has not been established. The aim was to establish the role of CSDs on the likelihood of living at home 30 days after discharge or being newly admitted to a care home.
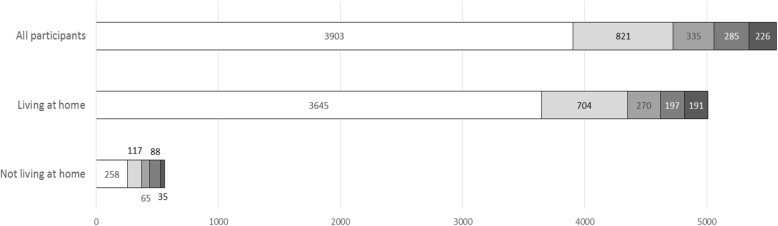
Methods: A prospective cohort study with routine data linkage was conducted based on admissions data from the acute medical unit of a district general hospital in Scotland. 5570 people aged ≥ 65 years admitted from a private residence who survived to discharge and received the Older Persons Routine Acute Assessment (OPRAA) during an incident emergency medical admission were included. The outcome measures were living at home, defined as a private residential address, 30 days after discharge and new care home admission at hospital discharge. Outcomes were ascertained through linkage to routine data sources.
Results: Of the 5570 individuals admitted from a private residence who survived to discharge, those without a CSD were more likely to be living at home at 30 days than those with a CSD (93.4% versus 81.7%; difference 11.7%, 95%CI 9.7-13.8%). New discharge to a care home affected 236 (4.2%) of the cohort, 181 (76.7%) of whom had a CSD. Logistic regression modelling identified that all four CSD categories were associated with a reduced likelihood of living at home and an increased likelihood of discharge to a care home. Those with delirium superimposed on dementia were the least likely to be living at home (OR 0.25), followed by those with dementia (OR 0.43), then unspecified cognitive impairment (OR 0.55) and finally delirium (OR 0.57).
Conclusions: Individuals with a CSD are at significantly increased risk of not returning home after hospitalisation, and those with CSDs account for the majority of new admissions to care homes on discharge. Individuals with delirium superimposed on dementia are the most affected. We need to understand how to configure and deliver healthcare services to enable older people to remain as independent as possible for as long as possible and to ensure transitions of care are managed supportively.
Keywords: Care home; Cognitive spectrum disorder; Data linkage; Delirium; Delirium superimposed on dementia; Dementia; Long-term care; Nursing home; Outcome.
Conflict of interest statement
Ethics approval and consent to participate
The University of Dundee Health Informatics Centre (HIC) performed the data linkage and provided an anonymised dataset in a secure Scottish Government accredited safe haven environment (HIC ISO27001) for analysis by the research team. HIC Standard Operating Procedures have been reviewed and approved by NHS East of Scotland Research Ethics Service. Permission for this project was granted by the NHS Fife Caldicott Guardian.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Imison C, Poteliakhoff E, Thompson J. Older people and emergency bed use—exploring variations. 2012.
-
- Wittenberg R, Sharpin L, McCormick L, Hurst J. Understanding emergency hospital admission of older people. 2015.
-
- Reynish EL, Hapca SM, De Souza N, Cvoro V, Donnan PT, Guthrie B. Epidemiology and outcomes of people with dementia, delirium, and unspecified cognitive impairment in the general hospital: prospective cohort study of 10,014 admissions. BMC Med. 2017;15(1):140. doi: 10.1186/s12916-017-0899-0. - DOI - PMC - PubMed
