

A cluster randomised controlled trial of two rounds of mass drug administration in Zanzibar, a malaria pre-elimination setting-high coverage and safety, but no significant impact on transmission
- PMID: 30526588
- PMCID: PMC6287359
- DOI: 10.1186/s12916-018-1202-8
A cluster randomised controlled trial of two rounds of mass drug administration in Zanzibar, a malaria pre-elimination setting-high coverage and safety, but no significant impact on transmission
Abstract
Background: Mass drug administration (MDA) has the potential to interrupt malaria transmission and has been suggested as a tool for malaria elimination in low-endemic settings. This study aimed to determine the effectiveness and safety of two rounds of MDA in Zanzibar, a pre-elimination setting.
Methods: A cluster randomised controlled trial was conducted in 16 areas considered as malaria hotspots, with an annual parasite index of > 0.8%. The areas were randomised to eight intervention and eight control clusters. The intervention included two rounds of MDA with dihydroartemisinin-piperaquine and single low-dose primaquine 4 weeks apart in May-June 2016. Primary and secondary outcomes were cumulative confirmed malaria case incidences 6 months post-MDA and parasite prevalences determined by PCR 3 months post-MDA. Additional outcomes included intervention coverage, treatment adherence, occurrence of adverse events, and cumulative incidences 3, 12, and 16 months post-MDA.
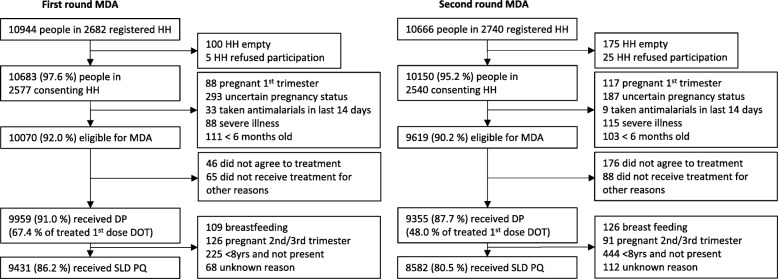
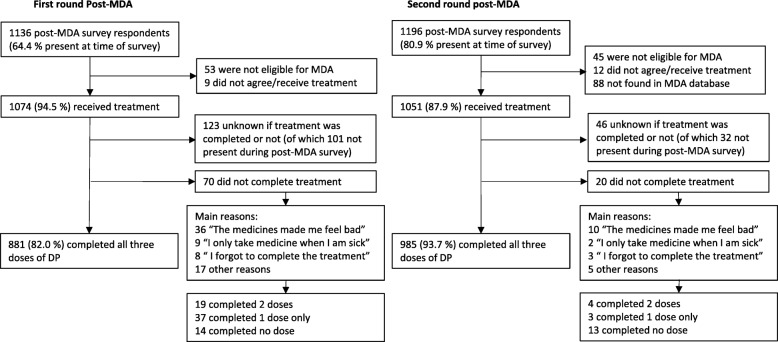
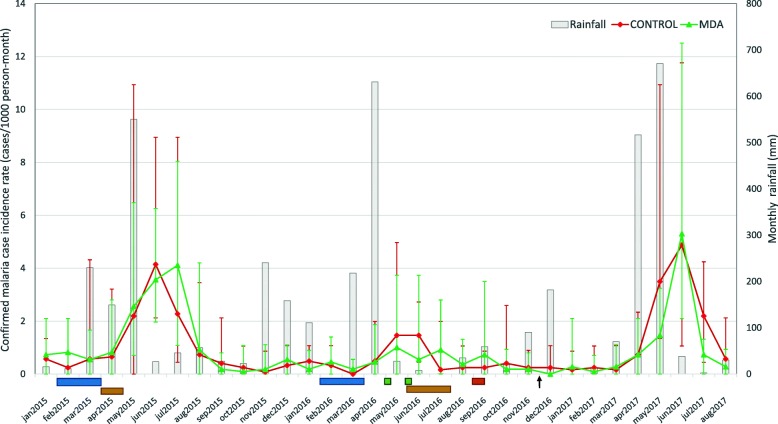
Results: Intervention coverage was 91.0% (9959/10944) and 87.7% (9355/10666) in the first and second rounds, respectively; self-reported adherence was 82.0% (881/1136) and 93.7% (985/1196). Adverse events were reported in 11.6% (147/1268) and 3.2% (37/1143) of post-MDA survey respondents after both rounds respectively. No serious adverse event was reported. No difference in cumulative malaria case incidence was observed between the control and intervention arms 6 months post-MDA (4.2 and 3.9 per 1000 population; p = 0.94). Neither was there a difference in PCR-determined parasite prevalences 3 months post-MDA (1.4% and 1.7%; OR = 1.0, p = 0.94), although having received at least the first MDA was associated with reduced odds of malaria infection (aOR = 0.35; p = 0.02). Among confirmed malaria cases at health facilities, 26.0% and 26.3% reported recent travel outside Zanzibar in the intervention and control shehias (aOR ≥ 85; p ≤ 0.001).
Conclusions: MDA was implemented with high coverage, adherence, and tolerability. Despite this, no significant impact on transmission was observed. The findings suggest that two rounds of MDA in a single year may not be sufficient for a sustained impact on transmission in a pre-elimination setting, especially when the MDA impact is restricted by imported malaria. Importantly, this study adds to the limited evidence for the use of MDA in low transmission settings in sub-Saharan Africa.
Trial registration: ClinicalTrials.gov, NCT02721186 (registration date: March 29, 2016).
Keywords: Adherence; Coverage; Dihydroartemisinin-piperaquine; Effectiveness; Elimination; Low transmission; Malaria; Mass drug administration; Safety; Single low-dose primaquine.
Conflict of interest statement
Ethics approval and consent to participate
Ethical approval was obtained from the Zanzibar Medical Research and Ethics Committee [ZAMREC/0001/January/2016] and the Zanzibar Food and Drugs Board [No.ZFDB/M.M:B:L:Z/16]. Verbal consent to conduct the study was sought from district authorities and from village leaders prior to the study onset. Written informed consent to participate in the study was sought from the head of household and household members over the age of 16 on the day of the first survey; it was made clear that individual participation in the study was voluntary. Ethical approval for molecular work at Karolinska Institutet was granted by the Regional Ethics Committee in Stockholm, Sweden [2013/836-32].
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Comment in
-
Mass drug administration for malaria elimination: do we understand the settings well enough?BMC Med. 2018 Dec 19;16(1):239. doi: 10.1186/s12916-018-1230-4. BMC Med. 2018. PMID: 30563509 Free PMC article.
References
-
- WHO . World malaria report. 2016.
-
- WHO . Mass drug administration, mass screening and treatment and focal screening and treatment for malaria: WHO Evidence Review Group meeting report. 2015.
-
- Cook Jackie, Xu Weiping, Msellem Mwinyi, Vonk Marlotte, Bergström Beatrice, Gosling Roly, Al-Mafazy Abdul-Wahid, McElroy Peter, Molteni Fabrizio, Abass Ali K., Garimo Issa, Ramsan Mahdi, Ali Abdullah, Mårtensson Andreas, Björkman Anders. Mass Screening and Treatment on the Basis of Results of a Plasmodium falciparum-Specific Rapid Diagnostic Test Did Not Reduce Malaria Incidence in Zanzibar. The Journal of Infectious Diseases. 2014;211(9):1476–1483. doi: 10.1093/infdis/jiu655. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
