

Microbial dysbiosis and mortality during mechanical ventilation: a prospective observational study
- PMID: 30526610
- PMCID: PMC6286574
- DOI: 10.1186/s12931-018-0950-5
Microbial dysbiosis and mortality during mechanical ventilation: a prospective observational study
Abstract
Background: Host-associated microbial communities have important roles in tissue homeostasis and overall health. Severe perturbations can occur within these microbial communities during critical illness due to underlying diseases and clinical interventions, potentially influencing patient outcomes. We sought to profile the microbial composition of critically ill mechanically ventilated patients, and to determine whether microbial diversity is associated with illness severity and mortality.
Methods: We conducted a prospective, observational study of mechanically ventilated critically ill patients with a high incidence of pneumonia in 2 intensive care units (ICUs) in Hamilton, Canada, nested within a randomized trial for the prevention of healthcare-associated infections. The microbial profiles of specimens from 3 anatomical sites (respiratory, and upper and lower gastrointestinal tracts) were characterized using 16S ribosomal RNA gene sequencing.
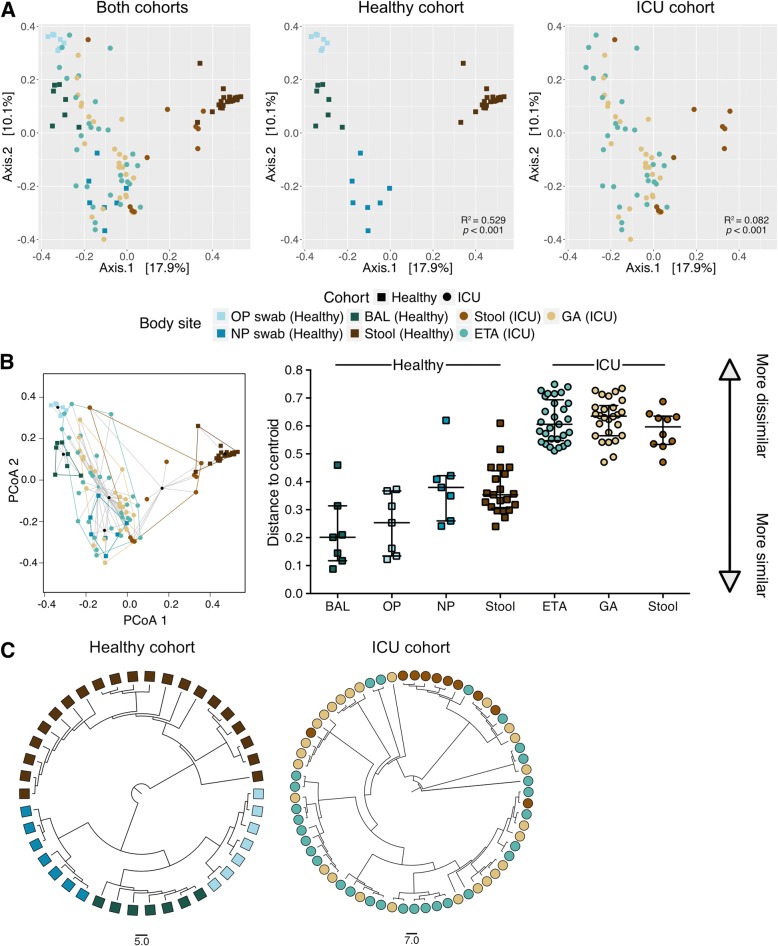
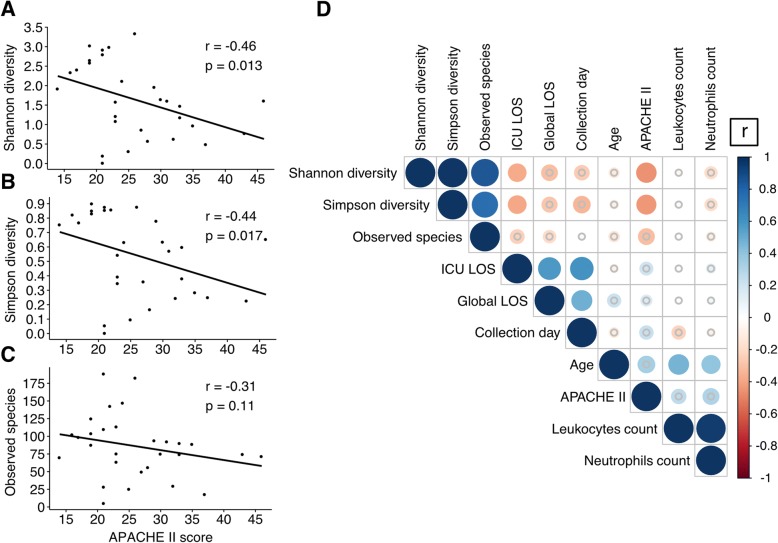
Results: We collected 65 specimens from 34 ICU patients enrolled in the trial (29 endotracheal aspirates, 26 gastric aspirates and 10 stool specimens). Specimens were collected at a median time of 3 days (lower respiratory tract and gastric aspirates; interquartile range [IQR] 2-4) and 6 days (stool; IQR 4.25-6.75) following ICU admission. We observed a loss of biogeographical distinction between the lower respiratory tract and gastrointestinal tract microbiota during critical illness. Moreover, microbial diversity in the respiratory tract was inversely correlated with APACHE II score (r = - 0.46, p = 0.013) and was associated with hospital mortality (Median Shannon index: Discharged alive; 1.964 vs. Deceased; 1.348, p = 0.045).
Conclusions: The composition of the host-associated microbial communities is severely perturbed during critical illness. Reduced microbial diversity reflects high illness severity and is associated with mortality. Microbial diversity may be a biomarker of prognostic value in mechanically ventilated patients.
Trial registration: ClinicalTrials.gov ID NCT01782755 . Registered February 4 2013.
Keywords: Critical illness; Gastrointestinal tract microbiota; Microbial diversity; Microbiome; Respiratory tract microbiota.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Hamilton Integrated Research Ethic Board (REB #13–170 and #13–238) and was performed in accordance with the principles of Good Clinical Practice following the Tri-Council guidelines. All participants or their substitute decision makers provided written informed consent prior to enrollment.
Consent for publication
Written contentment has been obtained for all participants or their substitute decision makers.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
