

Global patterns of mortality in international migrants: a systematic review and meta-analysis
- PMID: 30528484
- PMCID: PMC6294735
- DOI: 10.1016/S0140-6736(18)32781-8
Global patterns of mortality in international migrants: a systematic review and meta-analysis
Abstract
Background: 258 million people reside outside their country of birth; however, to date no global systematic reviews or meta-analyses of mortality data for these international migrants have been done. We aimed to review and synthesise available mortality data on international migrants.
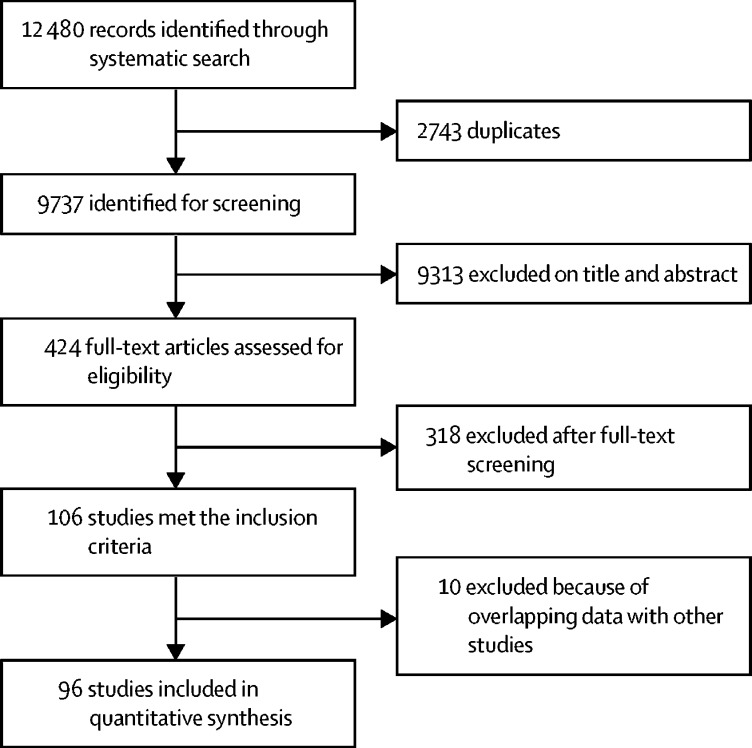
Methods: In this systematic review and meta-analysis, we searched MEDLINE, Embase, the Cochrane Library, and Google Scholar databases for observational studies, systematic reviews, and randomised controlled trials published between Jan 1, 2001, and March 31, 2017, without language restrictions. We included studies reporting mortality outcomes for international migrants of any age residing outside their country of birth. Studies that recruited participants exclusively from intensive care or high dependency hospital units, with an existing health condition or status, or a particular health exposure were excluded. We also excluded studies limited to maternal or perinatal outcomes. We screened studies using systematic review software and extracted data from published reports. The main outcomes were all-cause and International Classification of Diseases, tenth revision (ICD-10) cause-specific standardised mortality ratios (SMRs) and absolute mortality rates. We calculated summary estimates using random-effects models. This study is registered with PROSPERO, number CRD42017073608.
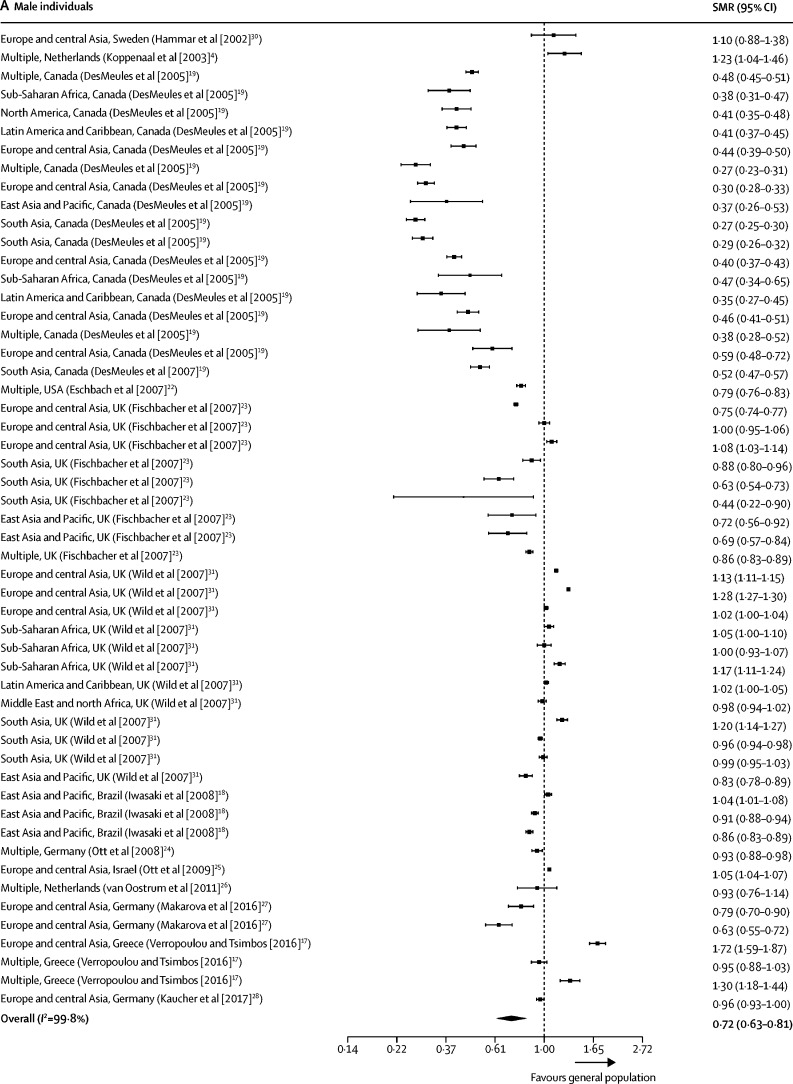
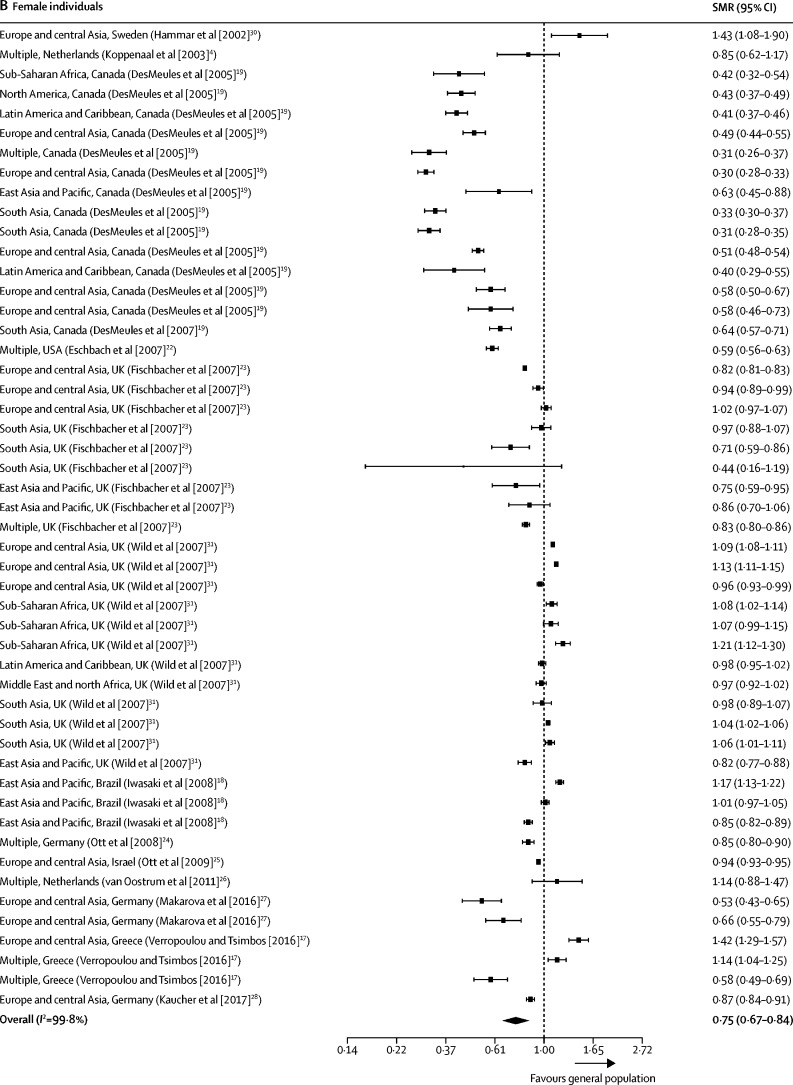
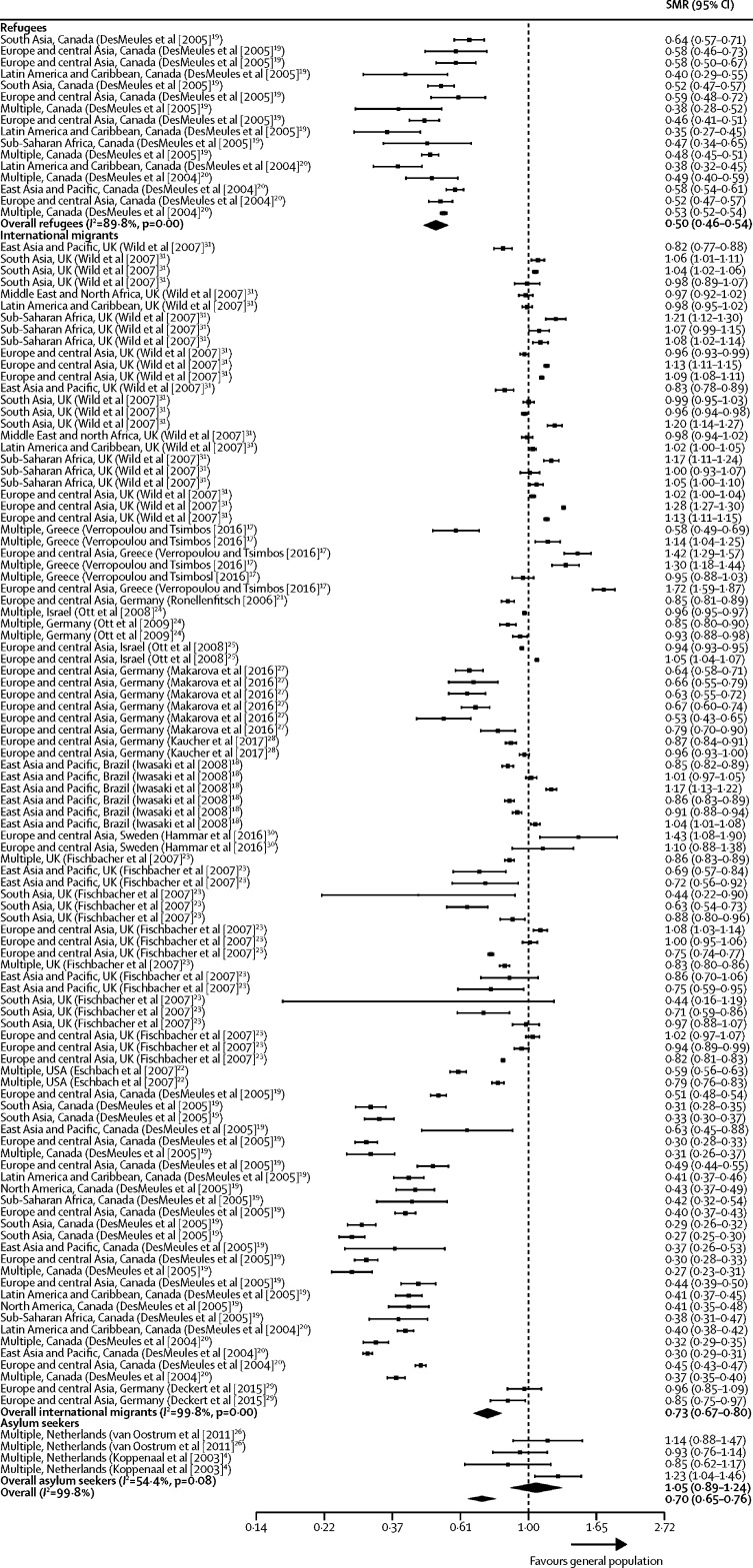
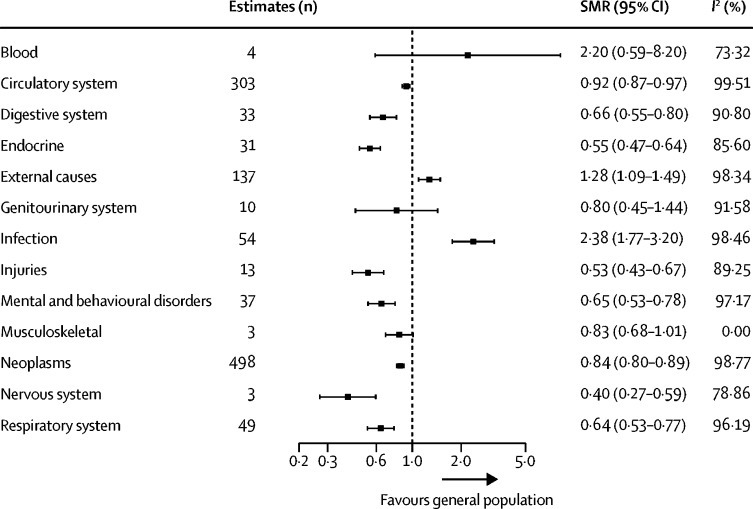
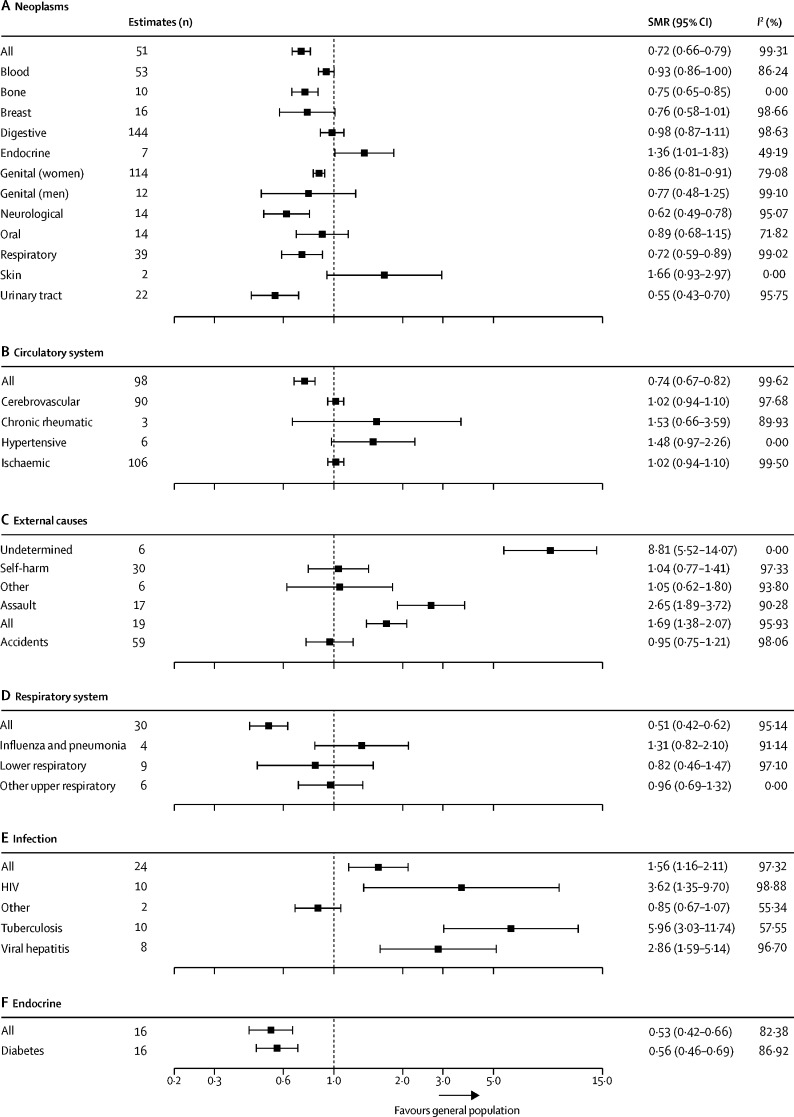
Findings: Of the 12 480 articles identified by our search, 96 studies were eligible for inclusion. The studies were geographically diverse and included data from all global regions and for 92 countries. 5464 mortality estimates for more than 15·2 million migrants were included, of which 5327 (97%) were from high-income countries, 115 (2%) were from middle-income countries, and 22 (<1%) were from low-income countries. Few studies included mortality estimates for refugees (110 estimates), asylum seekers (144 estimates), or labour migrants (six estimates). The summary estimate of all-cause SMR for international migrants was lower than one when compared with the general population in destination countries (0·70 [95% CI 0·65-0·76]; I2=99·8%). All-cause SMR was lower in both male migrants (0·72 [0·63-0·81]; I2=99·8%) and female migrants (0·75 [0·67-0·84]; I2=99·8%) compared with the general population. A mortality advantage was evident for refugees (SMR 0·50 [0·46-0·54]; I2=89·8%), but not for asylum seekers (1·05 [0·89-1·24]; I2=54·4%), although limited data was available on these groups. SMRs for all causes of death were lower in migrants compared with the general populations in the destination country across all 13 ICD-10 categories analysed, with the exception of infectious diseases and external causes. Heterogeneity was high across the majority of analyses. Point estimates of all-cause age-standardised mortality in migrants ranged from 420 to 874 per 100 000 population.
Interpretation: Our study showed that international migrants have a mortality advantage compared with general populations, and that this advantage persisted across the majority of ICD-10 disease categories. The mortality advantage identified will be representative of international migrants in high-income countries who are studying, working, or have joined family members in these countries. However, our results might not reflect the health outcomes of more marginalised groups in low-income and middle-income countries because little data were available for these groups, highlighting an important gap in existing research. Our results present an opportunity to reframe the public discourse on international migration and health in high-income countries.
Funding: Wellcome Trust, National Institute for Health Research, Medical Research Council, Alliance for Health Policy and Systems Research, Department for International Development, Fogarty International Center, Grand Challenges Canada, International Development Research Centre Canada, Inter-American Institute for Global Change Research, National Cancer Institute, National Heart, Lung and Blood Institute, National Institute of Mental Health, Swiss National Science Foundation, World Diabetes Foundation, UK National Institute for Health Research Imperial Biomedical Research Centre, Imperial College Healthcare Charity, and European Society for Clinical Microbiology and Infectious Diseases (ESCMID) Study Group Research Funding for the ESCMID Study Group for Infections in Travellers and Migrants.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Do migrants have a mortality advantage?Lancet. 2018 Dec 15;392(10164):2517-2518. doi: 10.1016/S0140-6736(18)33052-6. Epub 2018 Dec 5. Lancet. 2018. PMID: 30528483 No abstract available.
References
-
- UN Department of Economic and Social Affairs The International Migration Report 2017 (Highlights) https://www.un.org/development/desa/publications/international-migration...
-
- Razum O. Migrant mortality, healthy migrant effect. In: Kirch W, editor. Encyclopedia of public health. Springer; Dordrecht: 2008. pp. 932–935.
-
- McKay L, Macintyre S, Ellaway A. Migration and health: a review of the international literature. Medical Research Council Social and Public Health Sciences Unit. 2003. www.sphsu.mrc.ac.uk/library/occasional/OP012.pdf
-
- Koppenaal H, Bos CA, Broer J. High mortality due to infectious diseases and unnatural causes of death among asylum seekers in the Netherlands, 1998–1999. Ned Tijdschr Geneeskd. 2003;147:391–395. (in Dutch). - PubMed
Publication types
MeSH terms
Grants and funding
- P20 CA217231/CA/NCI NIH HHS/United States
- 206602/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- 209993/Z/17/Z/WT_/Wellcome Trust/United Kingdom
- MR/P008984/1/MRC_/Medical Research Council/United Kingdom
- 1P20CA217231/CA/NCI NIH HHS/United States
- U01 HL114180/HL/NHLBI NIH HHS/United States
- 5U01HL114180/HL/NHLBI NIH HHS/United States
- D71 TW010877/TW/FIC NIH HHS/United States
- 1UM1HL134590/HL/NHLBI NIH HHS/United States
- 205177/Z/16/Z/WT_/Wellcome Trust/United Kingdom
- MR/M007405/1/MRC_/Medical Research Council/United Kingdom
- HHSN268200900033C/HL/NHLBI NIH HHS/United States
- R21 TW009982/TW/FIC NIH HHS/United States
- MR/P02386X/1/MRC_/Medical Research Council/United Kingdom
- U19 MH098780/MH/NIMH NIH HHS/United States
- 1U19MH098780/MH/NIMH NIH HHS/United States
- UM1 HL134590/HL/NHLBI NIH HHS/United States
- MR/P024408/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
