

The UCL-Lancet Commission on Migration and Health: the health of a world on the move
- PMID: 30528486
- PMCID: PMC7612863
- DOI: 10.1016/S0140-6736(18)32114-7
The UCL-Lancet Commission on Migration and Health: the health of a world on the move
Abstract
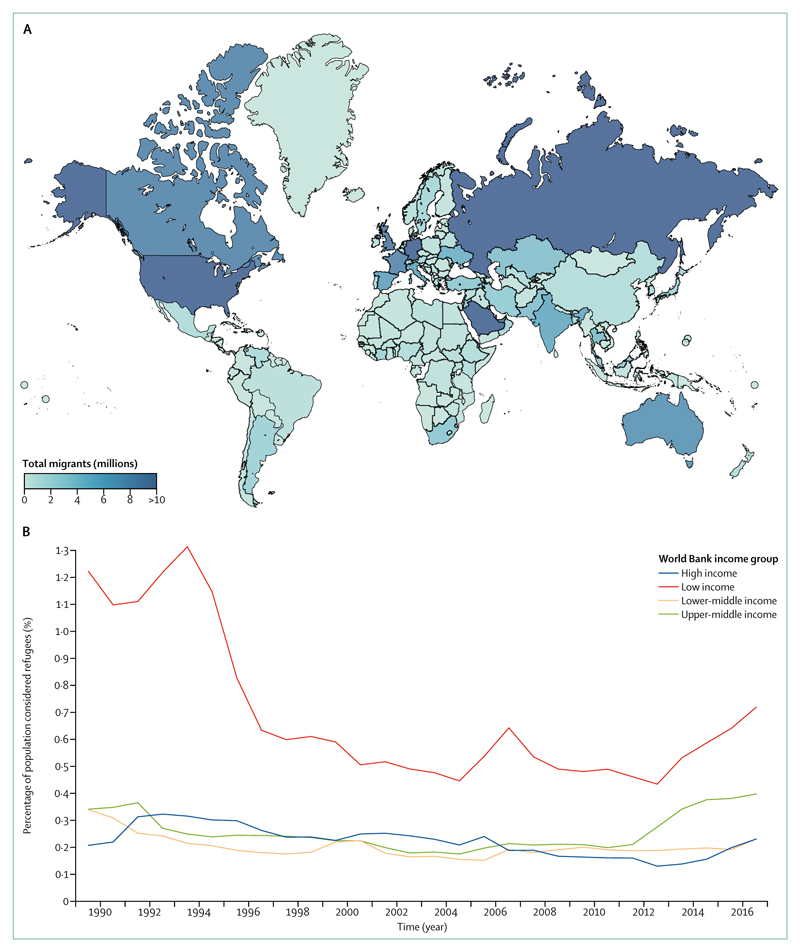
With one billion people on the move or having moved in 2018, migration is a global reality, which has also become a political lightning rod. Although estimates indicate that the majority of global migration occurs within low-income and middle-income countries (LMICs), the most prominent dialogue focuses almost exclusively on migration from LMICs to high-income countries (HICs). Nowadays, populist discourse demonises the very same individuals who uphold economies, bolster social services, and contribute to health services in both origin and destination locations. Those in positions of political and economic power continue to restrict or publicly condemn migration to promote their own interests. Meanwhile nationalist movements assert so-called cultural sovereignty by delineating an us versus them rhetoric, creating a moral emergency.
In response to these issues, the UCL-Lancet Commission on Migration and Health was convened to articulate evidence-based approaches to inform public discourse and policy. The Commission undertook analyses and consulted widely, with diverse international evidence and expertise spanning sociology, politics, public health science, law, humanitarianism, and anthropology. The result of this work is a report that aims to be a call to action for civil society, health leaders, academics, and policy makers to maximise the benefits and reduce the costs of migration on health locally and globally. The outputs of our work relate to five overarching goals that we thread throughout the report.
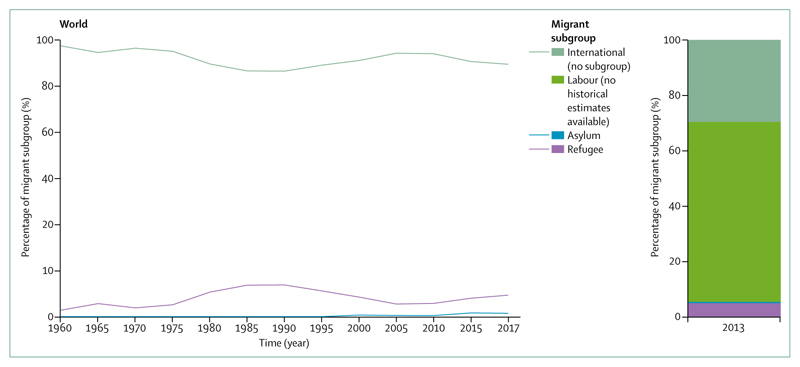
First, we provide the latest evidence on migration and health outcomes. This evidence challenges common myths and highlights the diversity, dynamics, and benefits of modern migration and how it relates to population and individual health. Migrants generally contribute more to the wealth of host societies than they cost. Our Article shows that international migrants in HICs have, on average, lower mortality than the host country population. However, increased morbidity was found for some conditions and among certain subgroups of migrants, (eg, increased rates of mental illness in victims of trafficking and people fleeing conflict) and in populations left behind in the location of origin. Currently, in 2018, the full range of migrants’ health needs are difficult to assess because of poor quality data. We know very little, for example, about the health of undocumented migrants, people with disabilities, or lesbian, gay, bisexual, transsexual, or intersex (LGBTI) individuals who migrate or who are unable to move.
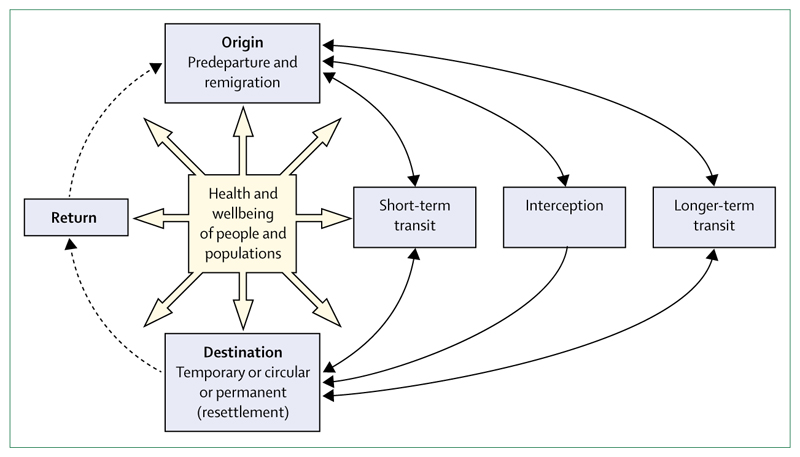
Second, we examine multisector determinants of health and consider the implication of the current sector-siloed approaches. The health of people who migrate depends greatly on structural and political factors that determine the impetus for migration, the conditions of their journey, and their destination. Discrimination, gender inequalities, and exclusion from health and social services repeatedly emerge as negative health influences for migrants that require cross-sector responses.
Third, we critically review key challenges to healthy migration. Population mobility provides economic, social, and cultural dividends for those who migrate and their host communities. Furthermore, the right to the highest attainable standard of health, regardless of location or migration status, is enshrined in numerous human rights instruments. However, national sovereignty concerns overshadow these benefits and legal norms. Attention to migration focuses largely on security concerns. When there is conjoining of the words health and migration, it is either focused on small subsets of society and policy, or negatively construed. International agreements, such as the UN Global Compact for Migration and the UN Global Compact on Refugees, represent an opportunity to ensure that international solidarity, unity of intent, and our shared humanity triumphs over nationalist and exclusionary policies, leading to concrete actions to protect the health of migrants.
Fourth, we examine equity in access to health and health services and offer evidence-based solutions to improve the health of migrants. Migrants should be explicitly included in universal health coverage commitments. Ultimately, the cost of failing to be health-inclusive could be more expensive to national economies, health security, and global health than the modest investments required.
Finally, we look ahead to outline how our evidence can contribute to synergistic and equitable health, social, and economic policies, and feasible strategies to inform and inspire action by migrants, policy makers, and civil society. We conclude that migration should be treated as a central feature of 21st century health and development. Commitments to the health of migrating populations should be considered across all Sustainable Development Goals (SDGs) and in the implementation of the Global Compact for Migration and Global Compact on Refugees. This Commission offers recommendations that view population mobility as an asset to global health by showing the meaning and reality of good health for all. We present four key messages that provide a focus for future action.
Conflict of interest statement
IA, DD, and RWA undertook paid consultancy work in support of the Doctors of the World 2017 Observatory report—Falling through the cracks: the failure of universal healthcare coverage in Europe. MO reports personal fees from WHO Regional Office for Europe, WHO Regional Office for the Eastern Mediterranean, Medecins Sans Frontieres, Operational Centre Brussels, outside the submitted work; and is a steering committee member for the Syria Public Health Network, which conducts research and policy work on public health issues in Syria and the region. All other authors declare no competing interests. The views and opinions expressed in this Article are those of the authors and do not necessarily reflect the views, official policy, or position of the International Organization for Migration, an organisation that is part of the UN system. The designations employed and the presentation of material throughout the article do not imply the expression of any opinion whatsoever on the part of the International Organization for Migration, concerning the legal status of any country, territory, city or area, or of its authorities, or concerning its frontiers or boundaries.
Figures

Comment in
-
The unmet needs of refugees and internally displaced people.Lancet. 2018 Dec 15;392(10164):2530-2532. doi: 10.1016/S0140-6736(18)32780-6. Epub 2018 Dec 5. Lancet. 2018. PMID: 30528475 No abstract available.
-
Bernadette Nirmal Kumar: making migrant health mainstream.Lancet. 2018 Dec 15;392(10164):2541. doi: 10.1016/S0140-6736(18)32936-2. Epub 2018 Dec 5. Lancet. 2018. PMID: 30528481 No abstract available.
-
Health of migrants: simple questions can improve care.Lancet. 2019 Jun 8;393(10188):2297-2298. doi: 10.1016/S0140-6736(19)30545-8. Epub 2019 May 20. Lancet. 2019. PMID: 31122667 No abstract available.
-
The UK National Health Service regulations for overseas visitors.Lancet. 2019 Aug 31;394(10200):734-735. doi: 10.1016/S0140-6736(19)31337-6. Lancet. 2019. PMID: 31478498 No abstract available.
-
Meeting the health challenges of displaced populations from Ukraine.Lancet. 2022 Mar 26;399(10331):1206-1208. doi: 10.1016/S0140-6736(22)00477-9. Epub 2022 Mar 11. Lancet. 2022. PMID: 35286844 Free PMC article. No abstract available.
References
-
- International Organization for Migration. [accessed June 25, 2018];World Migration Report. 2018 https://www.iom.int/wmr/world-migration-report-2018 .
-
- Urquia ML, Gagnon AJ. Glossary: migration and health. [accessed Jan 15, 2018];2011 - PubMed
-
- Major B, Dovidio JF, Link BG. The Oxford Handbook of Stigma, Discrimination, and Health. 2017. [accessed June 14, 2018]. https://books.google.com/books/about/The_Oxford_Handbook_of_Stigma_Discr... .
-
- Elliott P, Hennigan WJ. Exclusive: Navy document shows plan to erect ‘austere’ tent cities for immigrants. 2018. [accessed July 1, 2018]. http://time.com/5319334/navy-detainment-centers-zerol-tolerance-immigrat...
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
