

Acute respiratory failure in immunocompromised adults
- PMID: 30529232
- PMCID: PMC7185453
- DOI: 10.1016/S2213-2600(18)30345-X
Acute respiratory failure in immunocompromised adults
Abstract
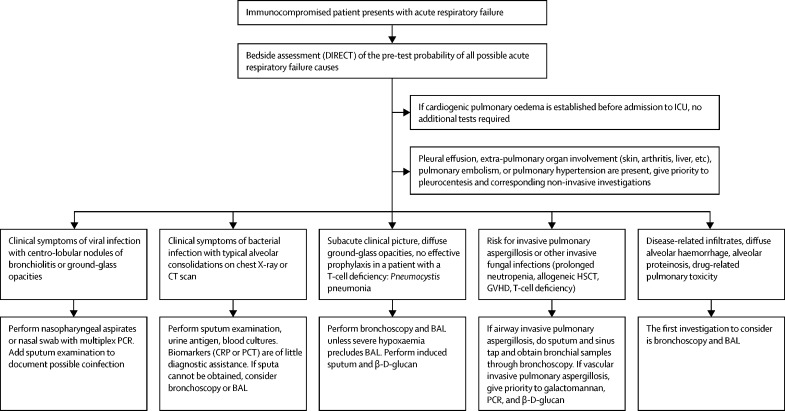
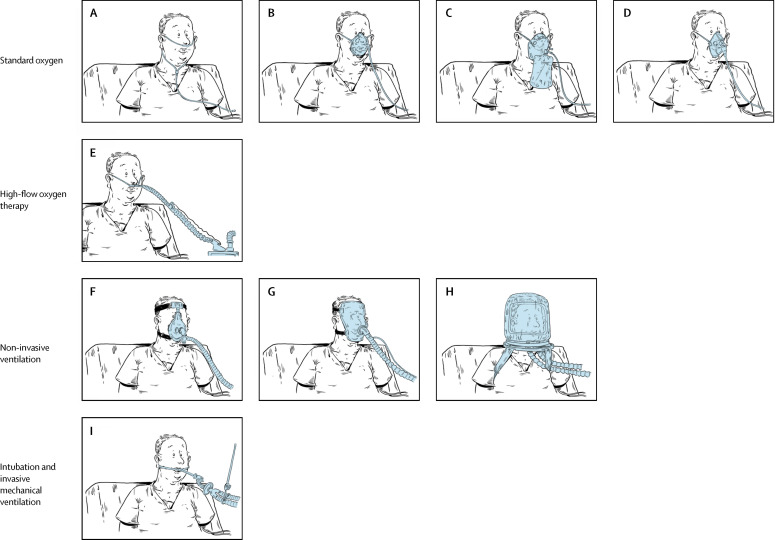
Acute respiratory failure occurs in up to half of patients with haematological malignancies and 15% of those with solid tumours or solid organ transplantation. Mortality remains high. Factors associated with mortality include a need for invasive mechanical ventilation, organ dysfunction, older age, frailty or poor performance status, delayed intensive care unit admission, and acute respiratory failure due to an invasive fungal infection or unknown cause. In addition to appropriate antibacterial therapy, initial clinical management aims to restore oxygenation and predict the most probable cause based on variables related to the underlying disease, acute respiratory failure characteristics, and radiographic findings. The cause of acute respiratory failure must then be confirmed using the most efficient, least invasive, and safest diagnostic tests. In patients with acute respiratory failure of undetermined cause, a standardised diagnostic investigation should be done immediately at admission before deciding whether to perform more invasive diagnostic procedures or to start empirical treatments. Collaborative and multidisciplinary clinical and research networks are crucial to improve our understanding of disease pathogenesis and causation and to develop less invasive diagnostic strategies and more targeted treatment options.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures
References
-
- Harpaz R, Dahl RM, Dooling KL. Prevalence of immunosuppression among US adults, 2013. JAMA. 2016;316:2547–2548. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. - PubMed
-
- Israni AK, Zaun D, Rosendale JD, Schaffhausen C, Snyder JJ, Kasiske BL. OPTN/SRTR 2016 annual data report: deceased organ donation. Am J Transplant. 2018;18(suppl 1):434–463. - PubMed
-
- Azoulay E, Thiéry G, Chevret S. The prognosis of acute respiratory failure in critically ill cancer patients. Medicine (Baltimore) 2004;83:360–370. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
