

The Fungal Cyp51-Specific Inhibitor VT-1598 Demonstrates In Vitro and In Vivo Activity against Candida auris
- PMID: 30530603
- PMCID: PMC6395925
- DOI: 10.1128/AAC.02233-18
The Fungal Cyp51-Specific Inhibitor VT-1598 Demonstrates In Vitro and In Vivo Activity against Candida auris
Abstract
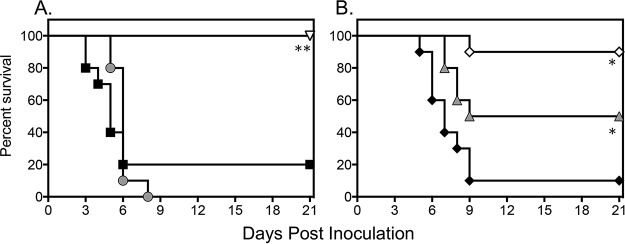
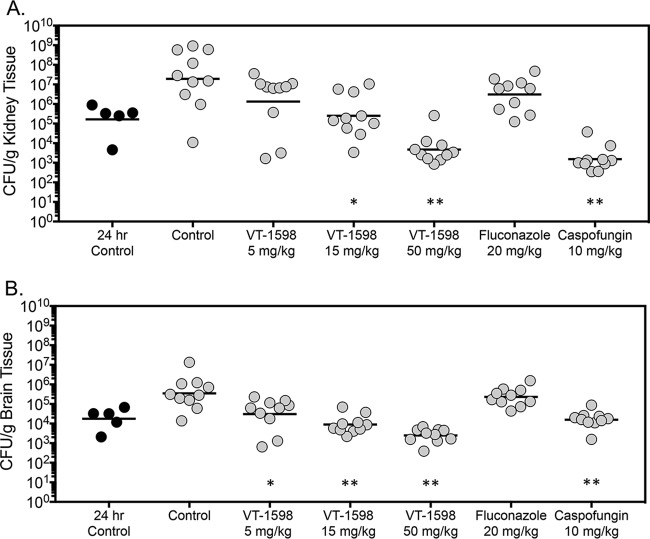
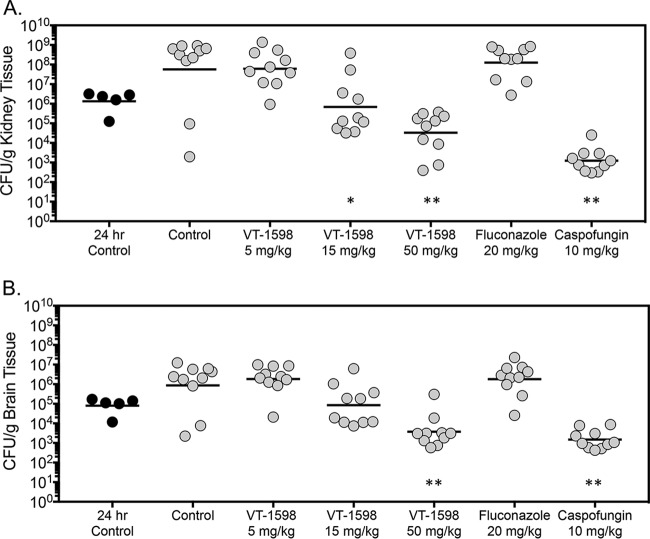
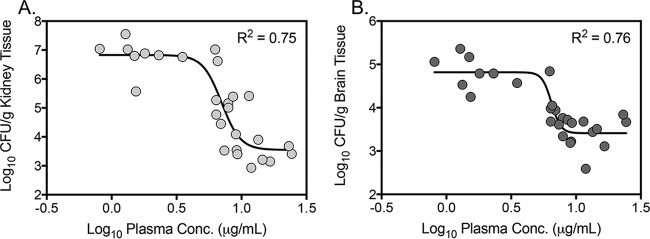
Candida auris is an emerging pathogen associated with significant mortality and often multidrug resistance. VT-1598, a tetrazole-based fungal CYP51-specific inhibitor, was evaluated in vitro and in vivo against C. auris Susceptibility testing was performed against 100 clinical isolates of C. auris by broth microdilution. Neutropenic mice were infected intravenously with C. auris, and treatment began 24 h postinoculation with a vehicle control, oral VT-1598 (5, 15, and 50 mg/kg of body weight once daily), oral fluconazole (20 mg/kg once daily), or intraperitoneal caspofungin (10 mg/kg once daily), which continued for 7 days. Fungal burden was assessed in the kidneys and brains on day 8 in the fungal burden arm and on the days the mice succumbed to infection or on day 21 in the survival arm. VT-1598 plasma trough concentrations were also assessed on day 8. VT-1598 demonstrated in vitro activity against C. auris, with a mode MIC of 0.25 μg/ml and MICs ranging from 0.03 to 8 μg/ml. Treatment with VT-1598 resulted in significant and dose-dependent improvements in survival (median survival, 15 and >21 days for VT-1598 at 15 and 50 mg/kg, respectively) and reductions in kidney and brain fungal burden (reductions of 1.88 to 3.61 log10 CFU/g) compared to the control (5 days). The reductions in fungal burden correlated with plasma trough concentrations. Treatment with caspofungin, but not fluconazole, also resulted in significant improvements in survival and reductions in fungal burden compared to those with the control. These results suggest that VT-1598 may be a future option for the treatment of invasive infections caused by C. auris.
Keywords: Candida auris; VT-1598; in vitro susceptibility; invasive candidiasis; murine model.
Copyright © 2019 American Society for Microbiology.
Figures
Similar articles
-
Efficacy of Delayed Therapy with Fosmanogepix (APX001) in a Murine Model of Candida auris Invasive Candidiasis.Antimicrob Agents Chemother. 2019 Oct 22;63(11):e01120-19. doi: 10.1128/AAC.01120-19. Print 2019 Nov. Antimicrob Agents Chemother. 2019. PMID: 31427304 Free PMC article.
-
Ibrexafungerp Demonstrates In Vitro Activity against Fluconazole-Resistant Candida auris and In Vivo Efficacy with Delayed Initiation of Therapy in an Experimental Model of Invasive Candidiasis.Antimicrob Agents Chemother. 2021 May 18;65(6):e02694-20. doi: 10.1128/AAC.02694-20. Print 2021 May 18. Antimicrob Agents Chemother. 2021. PMID: 33753333 Free PMC article.
-
The Novel Arylamidine T-2307 Demonstrates In Vitro and In Vivo Activity against Candida auris.Antimicrob Agents Chemother. 2020 Feb 21;64(3):e02198-19. doi: 10.1128/AAC.02198-19. Print 2020 Feb 21. Antimicrob Agents Chemother. 2020. PMID: 31844006 Free PMC article.
-
Candida auris and multidrug resistance: Defining the new normal.Fungal Genet Biol. 2019 Oct;131:103243. doi: 10.1016/j.fgb.2019.103243. Epub 2019 Jun 20. Fungal Genet Biol. 2019. PMID: 31228646 Free PMC article. Review.
-
Candida and candidaemia. Susceptibility and epidemiology.Dan Med J. 2013 Nov;60(11):B4698. Dan Med J. 2013. PMID: 24192246 Review.
Cited by
-
Hope on the Horizon: Novel Fungal Treatments in Development.Open Forum Infect Dis. 2020 Jan 12;7(2):ofaa016. doi: 10.1093/ofid/ofaa016. eCollection 2020 Feb. Open Forum Infect Dis. 2020. PMID: 32099843 Free PMC article. Review.
-
The evolution of antifungal therapy: Traditional agents, current challenges and future perspectives.Curr Res Microb Sci. 2025 Jan 11;8:100341. doi: 10.1016/j.crmicr.2025.100341. eCollection 2025. Curr Res Microb Sci. 2025. PMID: 39897698 Free PMC article. Review.
-
Safety and pharmacokinetics of antifungal agent VT-1598 and its primary metabolite, VT-11134, in healthy adult subjects: phase 1, first-in-human, randomized, double-blind, placebo-controlled study of single-ascending oral doses of VT-1598.Med Mycol. 2024 Mar 28;62(4):myae032. doi: 10.1093/mmy/myae032. Med Mycol. 2024. PMID: 38569652 Free PMC article. Clinical Trial.
-
Strategies to Better Target Fungal Squalene Monooxygenase.J Fungi (Basel). 2021 Jan 13;7(1):49. doi: 10.3390/jof7010049. J Fungi (Basel). 2021. PMID: 33450973 Free PMC article. Review.
-
Beyond Conventional Antifungals: Combating Resistance Through Novel Therapeutic Pathways.Pharmaceuticals (Basel). 2025 Mar 4;18(3):364. doi: 10.3390/ph18030364. Pharmaceuticals (Basel). 2025. PMID: 40143141 Free PMC article. Review.
References
-
- Lockhart SR, Etienne KA, Vallabhaneni S, Farooqi J, Chowdhary A, Govender NP, Colombo AL, Calvo B, Cuomo CA, Desjardins CA, Berkow EL, Castanheira M, Magobo RE, Jabeen K, Asghar RJ, Meis JF, Jackson B, Chiller T, Litvintseva AP. 2017. Simultaneous emergence of multidrug-resistant Candida auris on 3 continents confirmed by whole-genome sequencing and epidemiological analyses. Clin Infect Dis 64:134–140. doi:10.1093/cid/ciw691. - DOI - PMC - PubMed
-
- Tsay S, Welsh RM, Adams EH, Chow NA, Gade L, Berkow EL, Poirot E, Lutterloh E, Quinn M, Chaturvedi S, Kerins J, Black SR, Kemble SK, Barrett PM, Barton K, Shannon DJ, Bradley K, Lockhart SR, Litvintseva AP, Moulton-Meissner H, Shugart A, Kallen A, Vallabhaneni S, Chiller TM, Jackson BR. 2017. Notes from the field: ongoing transmission of Candida auris in health care facilities—United States, June 2016–May 2017. MMWR Morb Mortal Wkly Rep 66:514–515. doi:10.15585/mmwr.mm6619a7. - DOI - PMC - PubMed
-
- CDC. 2018. Tracking Candida auris. https://www.cdc.gov/fungal/candida-auris/tracking-c-auris.html. Accessed 10 October 2018.
-
- Kathuria S, Singh PK, Sharma C, Prakash A, Masih A, Kumar A, Meis JF, Chowdhary A. 2015. Multidrug-resistant Candida auris misidentified as Candida haemulonii: characterization by matrix-assisted laser desorption ionization–time of flight mass spectrometry and DNA sequencing and its antifungal susceptibility profile variability by Vitek 2, CLSI broth microdilution, and Etest method. J Clin Microbiol 53:1823–1830. doi:10.1128/JCM.00367-15. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
