

Survival among Veterans Obtaining Dialysis in VA and Non-VA Settings
- PMID: 30530657
- PMCID: PMC6317601
- DOI: 10.1681/ASN.2018050521
Survival among Veterans Obtaining Dialysis in VA and Non-VA Settings
Abstract
Background: Outcomes of veterans with ESRD may differ depending on where they receive dialysis and who finances this care, but little is known about variation in outcomes across different dialysis settings and financial arrangements.
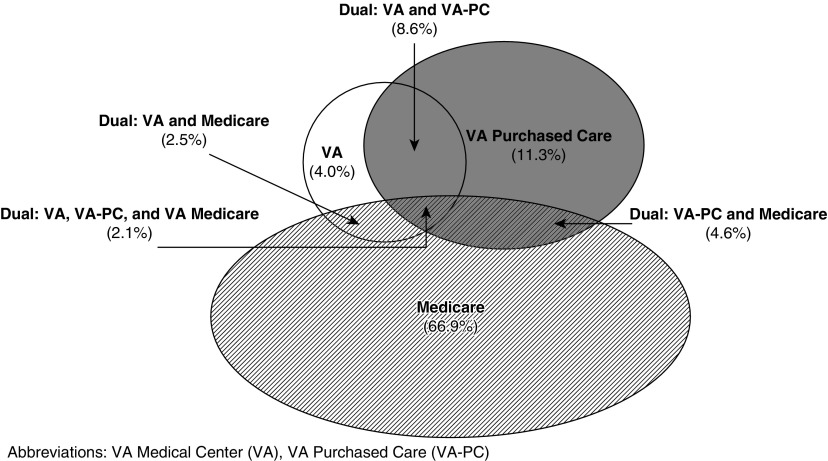
Methods: We examined survival among 27,241 Veterans Affairs (VA)-enrolled veterans who initiated chronic dialysis in 2008-2011 at (1) VA-based units, (2) community-based clinics through the Veterans Affairs Purchased Care program (VA-PC), (3) community-based clinics under Medicare, or (4) more than one of these settings ("dual" care). Using a Cox proportional hazards model, we compared all-cause mortality across dialysis settings during the 2-year period after dialysis initiation, adjusting for demographic and clinical characteristics.
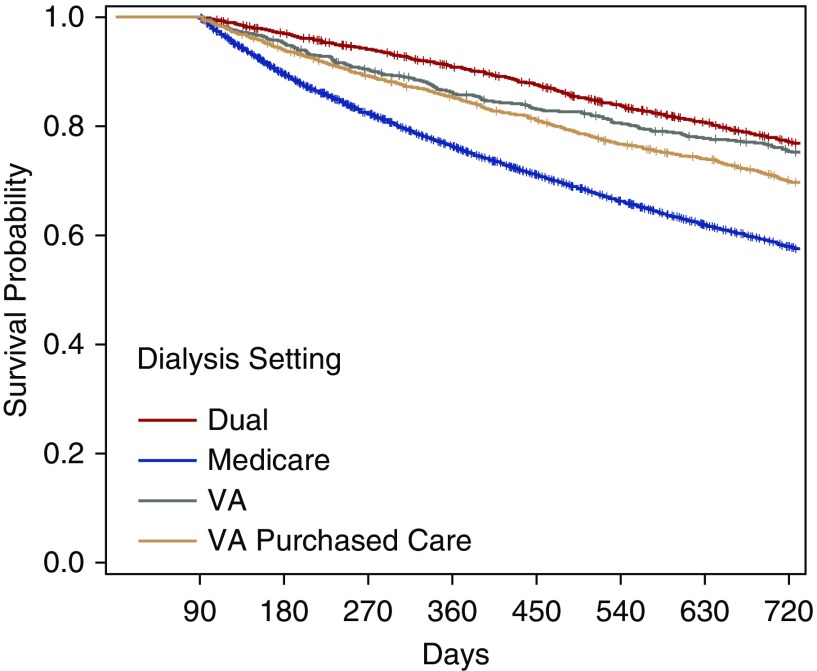
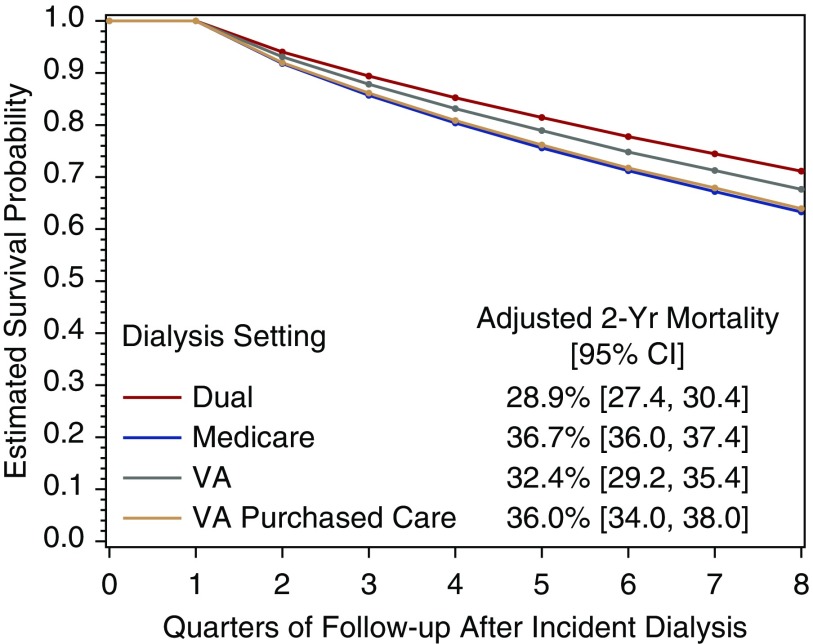
Results: Overall, 4% of patients received dialysis in VA, 11% under VA-PC, 67% under Medicare, and 18% in dual settings (nearly half receiving dual VA and VA-PC dialysis). Crude 2-year mortality was 25% for veterans receiving dialysis in the VA, 30% under VA-PC, 42% under Medicare, and 23% in dual settings. After adjustment, dialysis patients in VA or in dual settings had significantly lower 2-year mortality than those under Medicare; mortality did not differ in VA-PC and Medicare dialysis settings.
Conclusions: Mortality rates were highest for veterans receiving dialysis in Medicare or VA-PC settings and lowest for veterans receiving dialysis in the VA or dual settings. These findings inform institutional decisions about provision of dialysis for veterans. Further research identifying processes associated with improved survival for patients receiving VA-based dialysis may be useful in establishing best practices for outsourced veteran care.
Keywords: Medicare; Veterans Affairs; community care; dialysis; end-stage renal disease; mortality.
Copyright © 2019 by the American Society of Nephrology.
Figures
Comment in
-
Confounding of Race/Ethnicity and Age in the Survival among Veterans Obtaining Dialysis in VA and Non-VA Settings.J Am Soc Nephrol. 2019 Jul;30(7):1337. doi: 10.1681/ASN.2019030225. Epub 2019 May 16. J Am Soc Nephrol. 2019. PMID: 31097608 Free PMC article. No abstract available.
-
Authors' Reply.J Am Soc Nephrol. 2019 Jul;30(7):1338-1339. doi: 10.1681/ASN.2019040402. Epub 2019 May 16. J Am Soc Nephrol. 2019. PMID: 31097610 Free PMC article. No abstract available.
References
-
- Watnick S, Crowley ST: ESRD care within the US Department of Veterans Affairs: A forward-looking program with an illuminating past. Am J Kidney Dis 63: 521–529, 2014 - PubMed
-
- US Renal Data System (USRDS) : USRDS 2012 Annual Data Report: Atlas of End-Stage Renal Disease in the United States. Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases (NIH-NIDDK), 2012
-
- Veterans Health Administration : Allocation Resource Center: Fiscal Year 2011 Workload and Cost Report. Department of Veterans Affairs, Braintree, MA, 2012
-
- US Renal Data System (USRDS) : USRDS 2016 Annual Data Report, Volume 1: Chronic Kidney Disease in the United States. Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases (NIH-NIDDK), 2016
-
- Yoon J, Scott JY, Phibbs CS, Wagner TH: Recent trends in Veterans Affairs chronic condition spending. Popul Health Manag 14: 293–298, 2011 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
