

Personalized evidence based medicine: predictive approaches to heterogeneous treatment effects
- PMID: 30530757
- PMCID: PMC6889830
- DOI: 10.1136/bmj.k4245
Personalized evidence based medicine: predictive approaches to heterogeneous treatment effects
Abstract
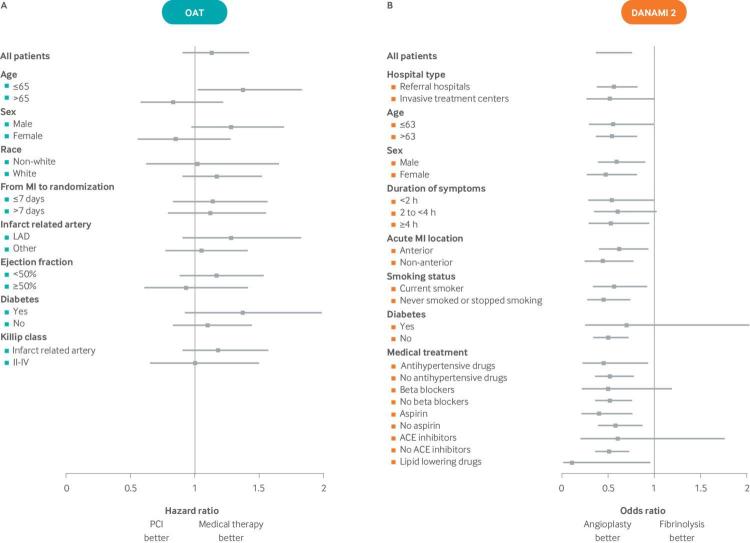
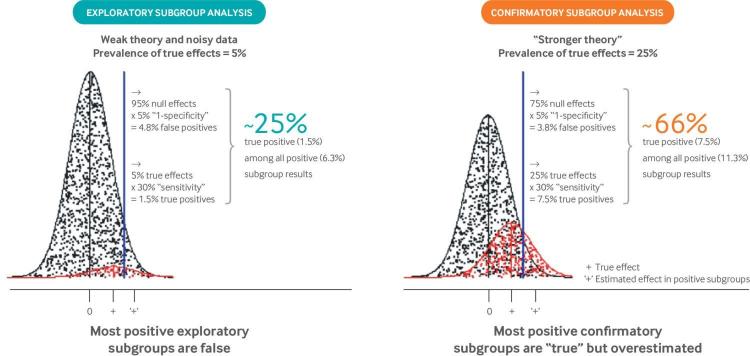
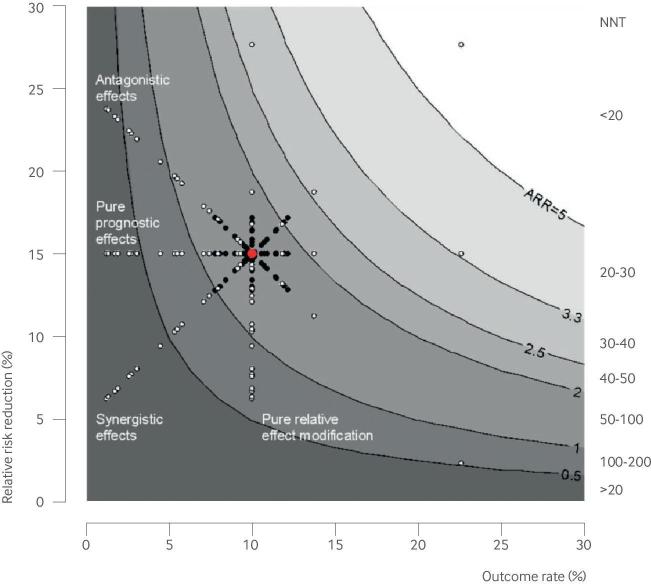
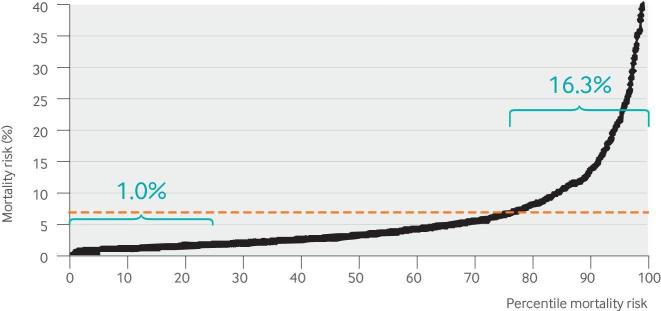
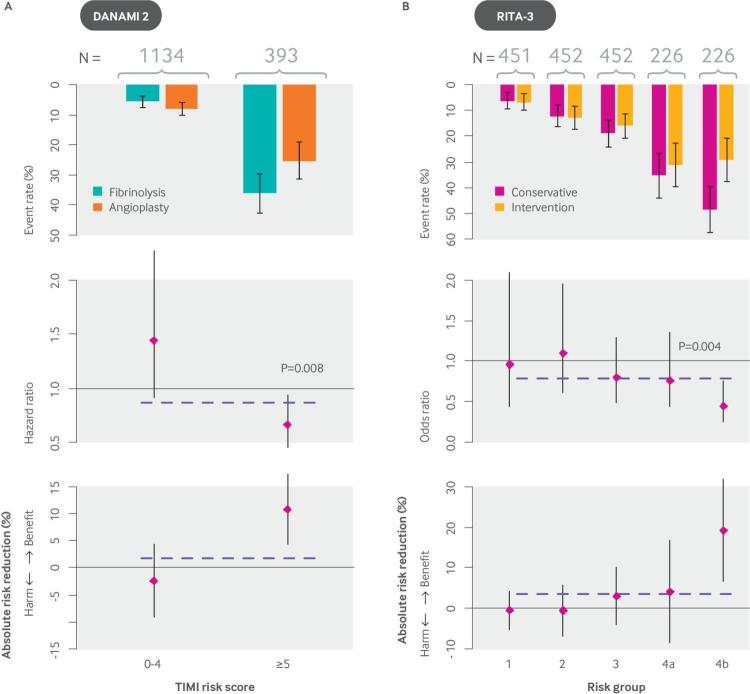
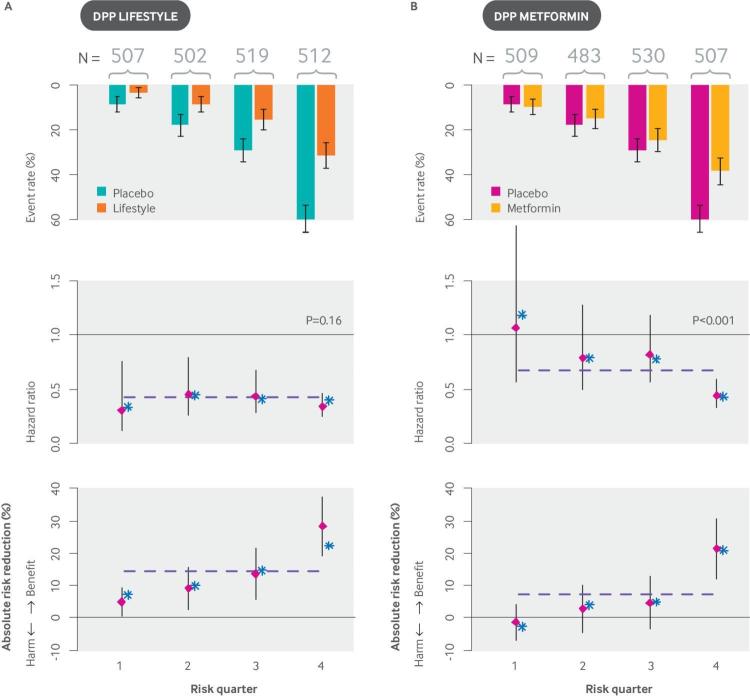
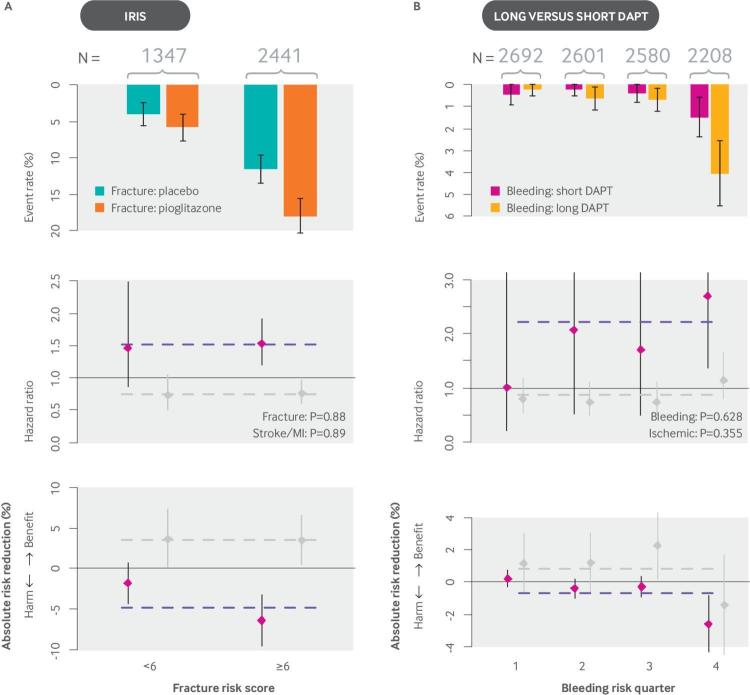
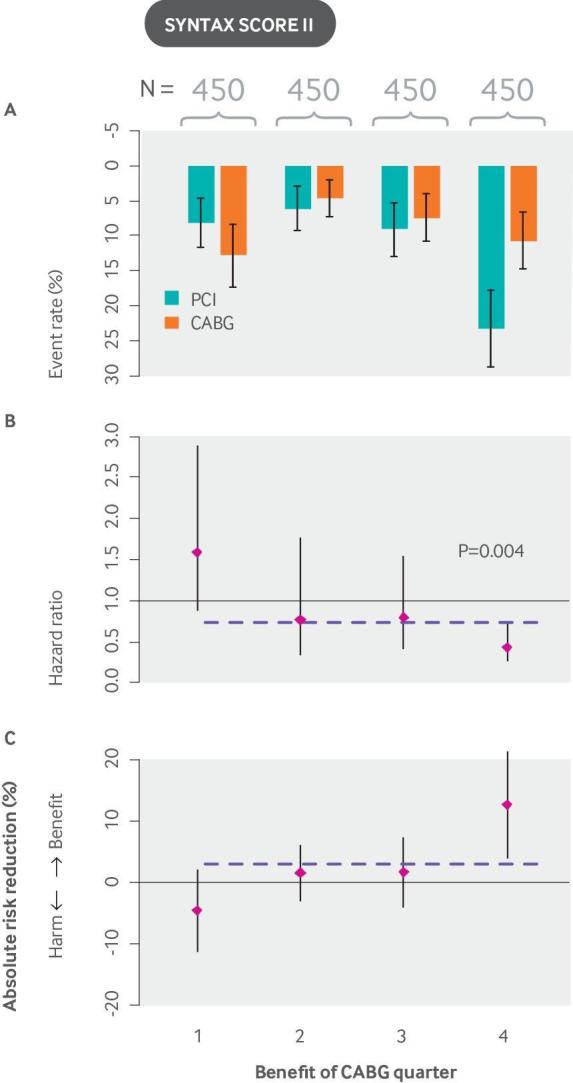
The use of evidence from clinical trials to support decisions for individual patients is a form of "reference class forecasting": implicit predictions for an individual are made on the basis of outcomes in a reference class of "similar" patients treated with alternative therapies. Evidence based medicine has generally emphasized the broad reference class of patients qualifying for a trial. Yet patients in a trial (and in clinical practice) differ from one another in many ways that can affect the outcome of interest and the potential for benefit. The central goal of personalized medicine, in its various forms, is to narrow the reference class to yield more patient specific effect estimates to support more individualized clinical decision making. This article will review fundamental conceptual problems with the prediction of outcome risk and heterogeneity of treatment effect (HTE), as well as the limitations of conventional (one-variable-at-a-time) subgroup analysis. It will also discuss several regression based approaches to "predictive" heterogeneity of treatment effect analysis, including analyses based on "risk modeling" (such as stratifying trial populations by their risk of the primary outcome or their risk of serious treatment-related harms) and analysis based on "effect modeling" (which incorporates modifiers of relative effect). It will illustrate these approaches with clinical examples and discuss their respective strengths and vulnerabilities.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have read and understood BMJ policy on declaration of interests and declare no competing interests.
Figures
References
-
- Kahneman D. Thinking, fast and slow. Farrar, Straus and Giroux, 2011.
-
- Kahneman D, Lovato L. Timid choices and bold forecasts: a cognitive perspective on risk taking. Manage Sci 1993;39:17-31 10.1287/mnsc.39.1.17. - DOI
-
- Meehl PE. Clinical versus statistical prediction: a theoretical analysis and a review of the evidence. University of Minnesota Press, 1954. 10.1037/11281-000 . - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources