

Can Dynamic Ultrasonography of the Hip Reliably Assess Anterior Femoral Head Translation?
- PMID: 30531425
- PMCID: PMC6494312
- DOI: 10.1097/CORR.0000000000000457
Can Dynamic Ultrasonography of the Hip Reliably Assess Anterior Femoral Head Translation?
Abstract
Background: Hip microinstability has gained attention recently as a potential cause of hip pain. Currently there is a lack of evidence-based objective diagnostic criteria surrounding this diagnosis. Previous studies have shown translation of the femoral head during extreme hip positions. However, reliable assessment of femoral head translation is lacking.
Questions/purposes: (1) How precise is musculoskeletal ultrasound for measuring anterior femoral head translation during the hip anterior apprehension test? (2) What is the intra- and interrater reliability of dynamic ultrasonography in assessing anterior femoral head translation?
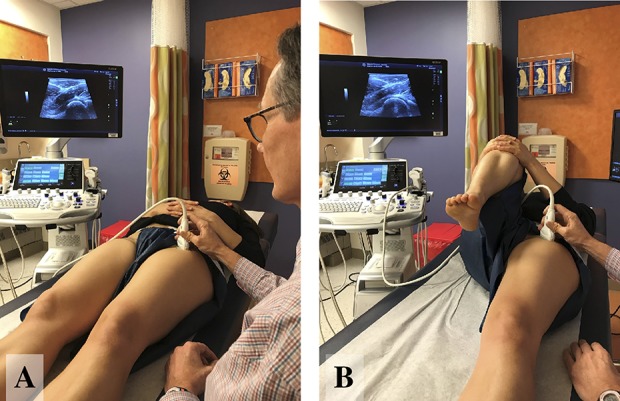
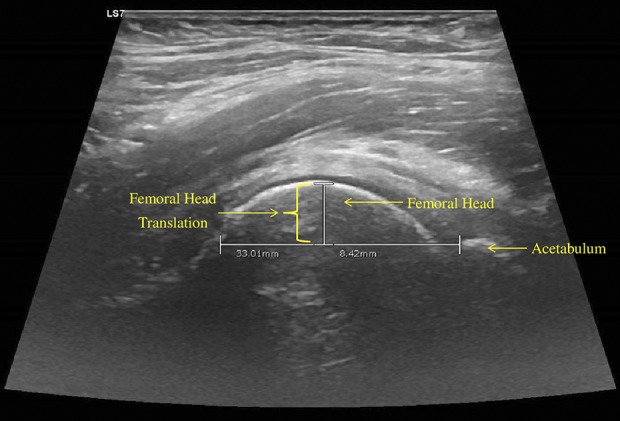
Methods: We recruited 10 study participants (20 hips) between the ages of 22 and 50 years with no history of hip pain or functional limitations. Test-retest methodology was used. Seven females and three males were enrolled. The mean age of study participants was 27 years (SD 8.7 years); mean body mass index was 22.6 kg/m (SD 2.2 kg/m). All study participants underwent dynamic hip ultrasonography by three different physicians 1 week apart. Each hip was visualized in two neutral positions (neutral and neutral with the contralateral hip flexed [NF]) and two dynamic positions, which sought to replicate the apprehension test, although notably study participants had no known hip pathology and therefore no apprehension. The first maintained the hip in extension and external rotation off to the side of the examination table (EER1), and the second held the hip off of the bottom of the examination table (EER2). One hundred twenty ultrasound scans (480 images) were performed. Mean and SD were calculated using absolute values of the difference in ultrasound measurements (mm) between positions NF and EER1 and NF and EER2 calculated for each physician as well as an average of all three physicians. Intraclass correlation coefficient (ICC) analysis was used to examine intra- and interrater reliability.
Results: The mean absolute difference for NF and EER1 was 0.84 mm (SD 0.93 mm) and for NF and EER2 0.62 mm (SD 0.40 mm) on Study Day 1. Similarly, on Study Day 2, the mean absolute difference for NF and EER1 position was 0.90 mm (SD 0.74 mm) and for NF and EER2 1.03 mm (SD 1.18 mm). Cumulative values of ICC analysis indicated excellent intrarater reliability in all four positions: neutral 0.794 (95% confidence interval [CI], 0.494-0.918), NF 0.927 (95% CI, 0.814-0.971), EER1 0.929 (95% CI, 0.825-0.972), and EER2 0.945 (95% CI, 0.864-0.978). Similarly, interrater ICC analysis cumulative values were excellent for NF, EER1, and EER2 and fair to good for the neutral position: neutral 0.725 (95% CI, 0.526-0.846), NF 0.846 (95% CI, 0.741-0.913), EER1 0.812 (95% CI, 0.674-0.895), and EER2 0.794 (95% CI, 0.652-0.884).
Conclusions: This study offers the first ultrasound protocol of which we are aware for measuring anterior femoral head translation. Hip dynamic ultrasound may assist in providing precise objective clinical-based diagnostic evidence when evaluating complex hip pain and suspected microinstability. Musculoskeletal ultrasound is a reliable office-based method of measuring anterior femoral head translation that can be utilized by physicians with varying experience levels. Future studies are needed to investigate ultrasound anterior femoral head translation taking into account sex, prior hip surgery, hip osseous morphology, and ligamentous laxity.
Level of evidence: Level III, diagnostic study.
Conflict of interest statement
Each author certifies that neither he or she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and
Figures

Comment in
-
CORR Insights®: Can Dynamic Ultrasonography of the Hip Reliably Assess Anterior Femoral Head Translation?Clin Orthop Relat Res. 2019 May;477(5):1099-1100. doi: 10.1097/CORR.0000000000000500. Clin Orthop Relat Res. 2019. PMID: 30247234 Free PMC article. No abstract available.
References
-
- Abrams GD, Luria A, Sampson J, Madding RA, Robinson WH, Safran MR, Sokolove J. Decreased synovial inflammation in atraumatic hip microinstability compared with femoroacetabular impingement. Arthroscopy. 2017;33:553–558. - PubMed
-
- Borsa PA, Scibek JS, Jacobson JA, Meister K. Sonographic stress measurement of glenohumeral joint laxity in collegiate swimmers and age-matched controls. Am J Sports Med. 2005;33:1077–1084. - PubMed
-
- Boykin RE, Anz AW, Bushnell BD, Kocher MS, Stubbs AJ, Philippon MJ. Hip instability. J Am Acad Orthop Surg. 2011;19:340–349. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
