

Buprenorphine Pharmacology Review: Update on Transmucosal and Long-acting Formulations
- PMID: 30531584
- PMCID: PMC7442141
- DOI: 10.1097/ADM.0000000000000457
Buprenorphine Pharmacology Review: Update on Transmucosal and Long-acting Formulations
Abstract
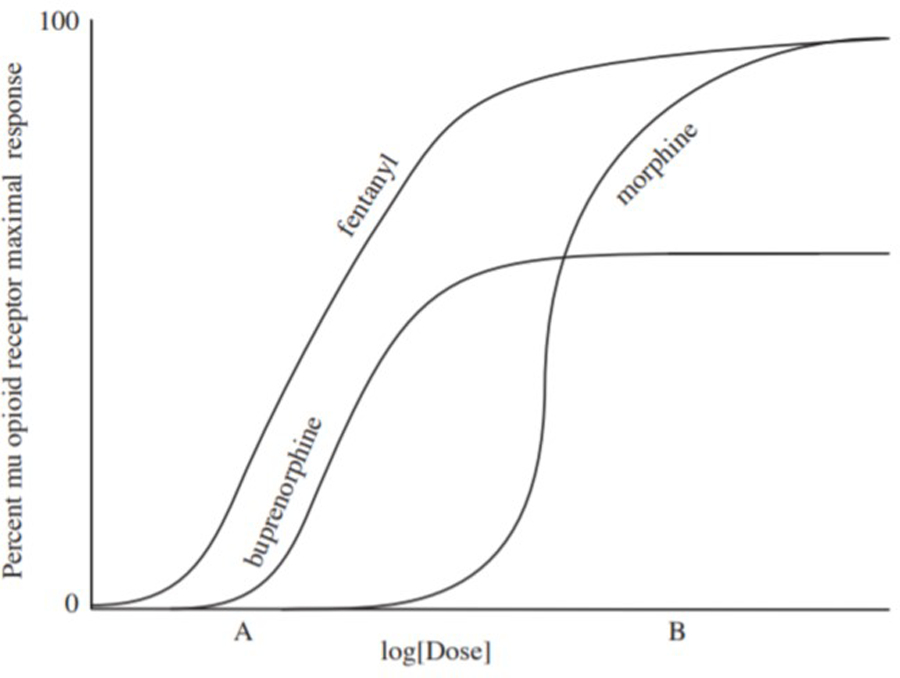
: Buprenorphine is an effective treatment for opioid use disorder. As a high-affinity, partial agonist for the mu-opioid receptor, buprenorphine suppresses opioid withdrawal and craving, reduces illicit opioid use, and blocks exogenous opioid effects including respiratory depression. Other pharmacologic benefits of buprenorphine are its superior safety profile compared with full opioid agonists and its long half-life that allows daily or less-than-daily dosing. New and innovative buprenorphine formulations, with pharmacokinetic profiles that differ from the original tablet formulation, continue to be developed. These include higher bioavailability transmucosal tablets and films and also 6-month implantable and monthly injectable products. This growing array of available formulations allows more choices for patients and increased opportunity for clinicians to individualize treatment; thus, it is important for buprenorphine prescribers to understand these differences.
Conflict of interest statement
Figures
References
-
- U.S. Food and Drug Administration/Center for Drug Evaluation and Research. Clinical Pharmacology and Biopharmaceutics Review: Suboxone® (Buprenorphine HCl/Naloxone HCl) 2mg/0.5mg, 8mg/2mg Sublingual Tablets. September 10, 2002.
-
- Amass L, Bickel WK, Higgins ST, Badger GJ. Alternate-day dosing during buprenorphine treatment of opioid dependence. Life Sci 1994;54:1215–28. - PubMed
-
- The American Society of Addiction Medicine. Public Policy Statement on Morphine Equivalent Units/Morphine Milligram Equivalents. Available at: https://www.asam.org/advocacy/find-a-policy-statement/view-policy-statem.... Accessed December 10, 2017.
-
- Auriacombe M, O’Brien CP, Tignol J. Buprenorphine in the treatment of opiate dependence. Ann Med Interne (Paris) 1994;145 Suppl 3:27. - PubMed
-
- Bickel WK, Amass L, Crean JP, Badger GJ. Buprenorphine dosing every 1, 2, or 3 days in opioid-dependent patients. Psychopharmacology (Berl) 1999;146:111–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
