

A randomized controlled trial of a transdiagnostic cognitive-behavioral intervention for Afro-descendants' survivors of systemic violence in Colombia
- PMID: 30532155
- PMCID: PMC6287825
- DOI: 10.1371/journal.pone.0208483
A randomized controlled trial of a transdiagnostic cognitive-behavioral intervention for Afro-descendants' survivors of systemic violence in Colombia
Abstract
Background: Exposure to violence has negative consequences on mental health. Armed-conflict in Colombia has widely affected Afro-descendants in the Pacific region. Evidence regarding effectiveness of mental health interventions is lacking in low-income settings, especially in areas with active conflict. The objective of this study is to evaluate an individualized Common Elements Treatment Approach (CETA), a transdiagnostic psychotherapy model based on Cognitive-Behavioral Therapy, for adult trauma survivors.
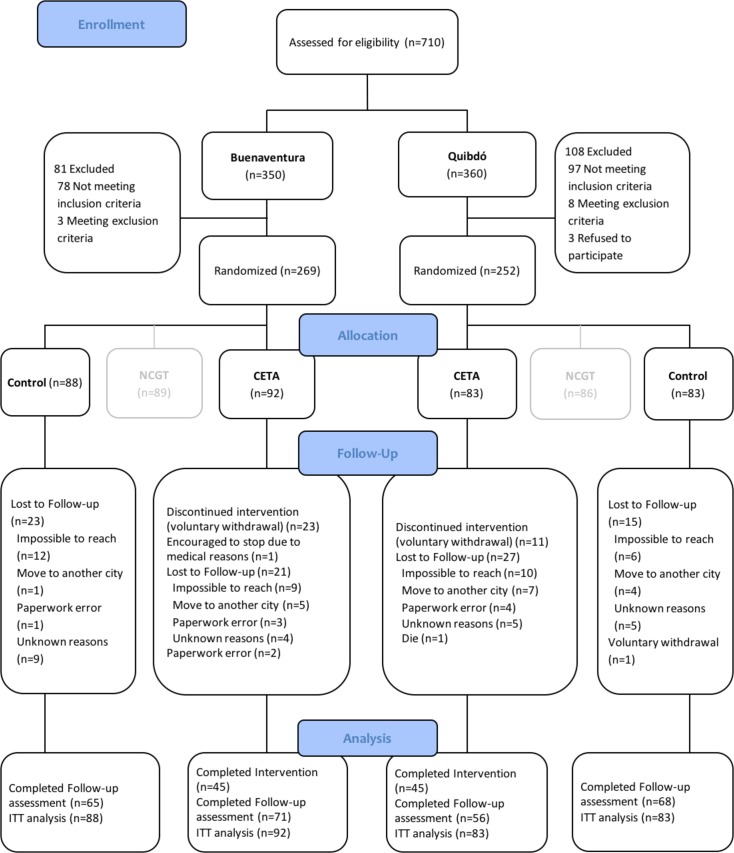
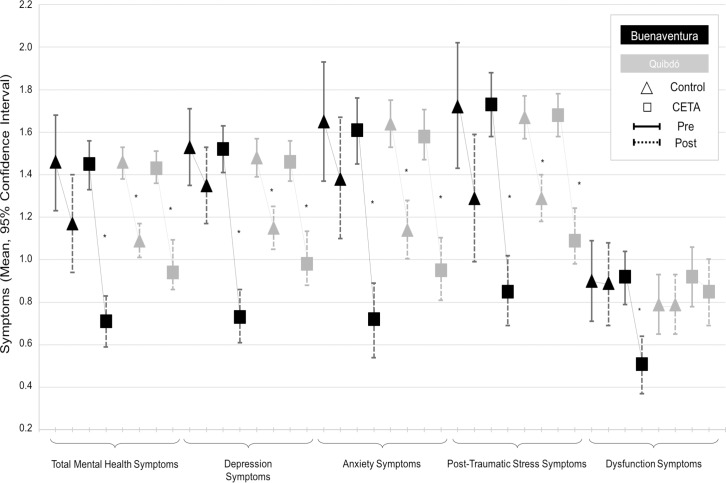
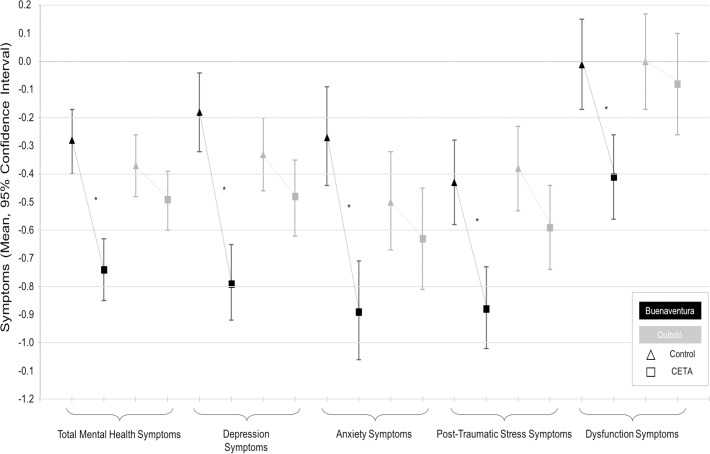
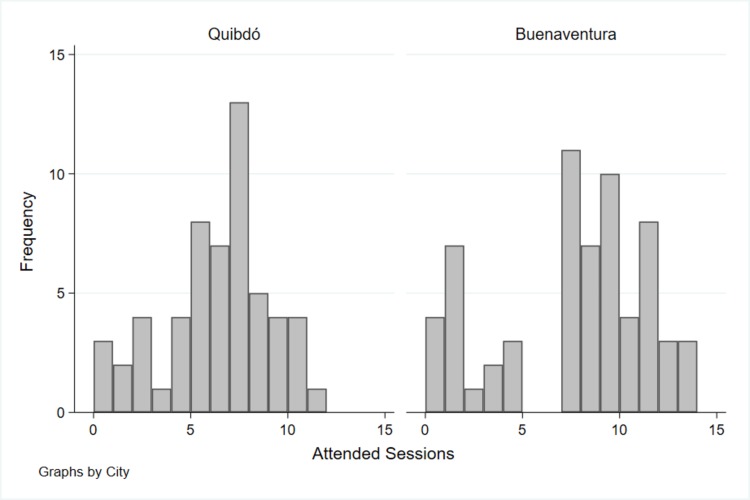
Methods and findings: A referred sample of 521 adult Afro-descendants from Buenaventura and Quibdó, Colombia, experiencing significant sadness, suffering or fear (score>0.77 in Total Mental Health Symptoms), with history of traumatic experiences, and with associated functional impairment were randomly allocated to CETA intervention, standby group without intervention, but under monthly monitoring, or a Narrative Community-Based Group Therapy. CETA was provided by trained Lay Psychosocial Community Workers without previous mental health experience, supervised by psychologists, during 12-14 weekly, 1.5-hour sessions. Symptoms were assessed with a locally validated survey built based on the Hopkins Symptom Checklist, the Harvard Trauma Questionnaire, the PTSD CheckList-Civilian Version, a qualitative study for additional general symptoms and a gender-specific functional impairment scale. CETA was compared with the control group and the intervention effects were calculated with mixed models using intention to treat analysis. Participant completion of follow-up was 75.1% and 13.2% voluntarily withdrew. Reduction in post-traumatic stress symptoms was significant in both municipalities when comparing intervention and control groups (mean difference), with a with a moderate effect size in Buenaventura (Cohen's d = 0.70) and a small effect size in Quibdó (d = 0.31). In Buenaventura, the intervention also had significant effects on depression (large effect size d = 1.03), anxiety (large effect size d = 0.80) and functional impairment (moderate effect size d = 0.70). In Quibdó, it had no significant effect on these outcomes. Changes in Total Mental Health Symptoms were not significant in neither city.
Conclusions: This trial suggests that CETA, can be effective in improving depression, anxiety, post-traumatic stress and function among victims of systematized violence in low-income and active conflict settings. Nonetheless, the difference of effectiveness between the two cities of intervention may indicate that we cannot assume that a mental health intervention known to be effective in one setting will be effective in another, even in similar circumstances and population. This may have special importance when implementing and reproducing these types of intervention in non-controlled circumstances. Further research should address these concerns. Results can be of use by governmental decision-makers when defining mental health programs for survivors.
Trial registration: ClinicalTrials.gov NCT01856673 (https://clinicaltrials.gov/ct2/show/NCT01856673).
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Internal Displacement Monitoring Centre—IDMC, Norwegian Refugee Council—NRC. Global Report on Internal Displacement GRID 2018. Geneva: IDMC, 2018 May 2018. Report No.
-
- Colombian Government, Unit for Victims. Official Victims' Registry Bogota D.C.: Colombian Government,; 2018 [updated Sep 1, 2018; cited 2018 Sept 13]. Available from: https://www.unidadvictimas.gov.co/es/registro-unico-de-victimas-ruv/37394.
-
- Albuja S, Arnaud E, Caterina M, Charron G, Foster F, Glatz AK, et al. Global Overview 2014: People Internally Displaced by Conflict and Violence. Geneva: Internal Displacement Monitoring Centre. Norwegian Refugee Council; 2014. 78 p.
-
- Franco Agudelo S. [Violence and Health in Colombia]. [Proceedings of the National Health Sector Forum Against Violence in Colombia: Policy and Plan of Action organized by the Ministry of Health and the Health and Development Corporation]. Bogota D.C: Ministry of Health; 1998. p. 27–39.
-
- Krug E, Dahlberg L, Mercy J, Zwi A, Lozano R. World Report on Violence and Health. Geneva: World Health Organization, 2002.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
