

Safety and efficacy of the rSh28GST urinary schistosomiasis vaccine: A phase 3 randomized, controlled trial in Senegalese children
- PMID: 30532268
- PMCID: PMC6300301
- DOI: 10.1371/journal.pntd.0006968
Safety and efficacy of the rSh28GST urinary schistosomiasis vaccine: A phase 3 randomized, controlled trial in Senegalese children
Abstract
Background: Urinary schistosomiasis, the result of infection by Schistosoma haematobium (Sh), remains a major global health concern. A schistosome vaccine could represent a breakthrough in schistosomiasis control strategies, which are presently based on treatment with praziquantel (PZQ). We report the safety and efficacy of the vaccine candidate recombinant 28-kDa glutathione S-transferase of Sh (rSh28GST) designated as Bilhvax, in a phase 3 trial conducted in Senegal.
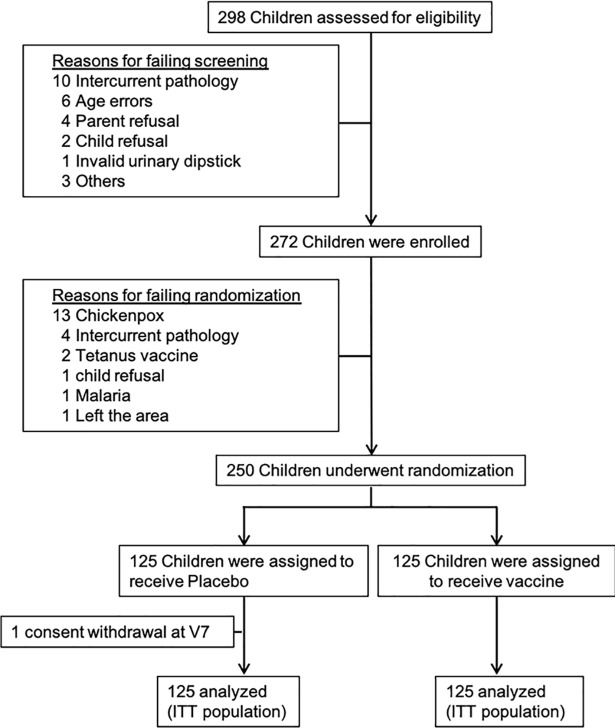
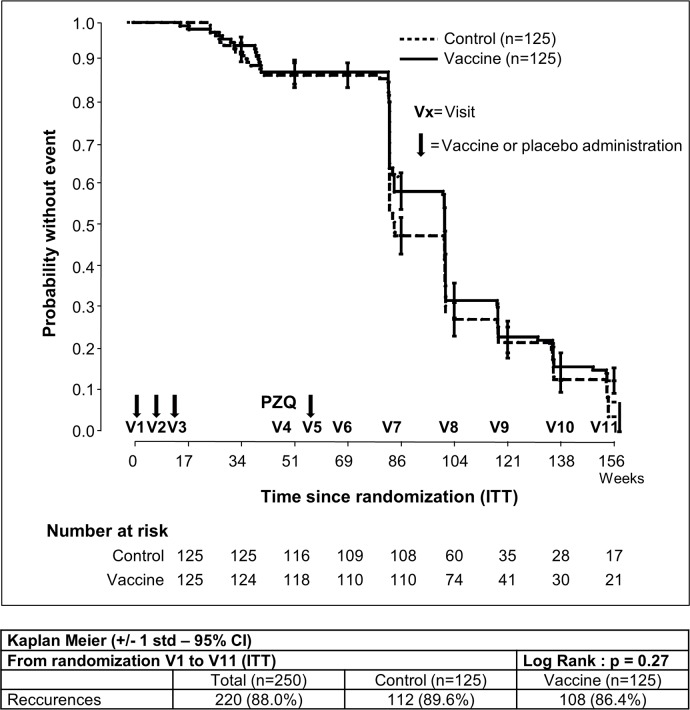
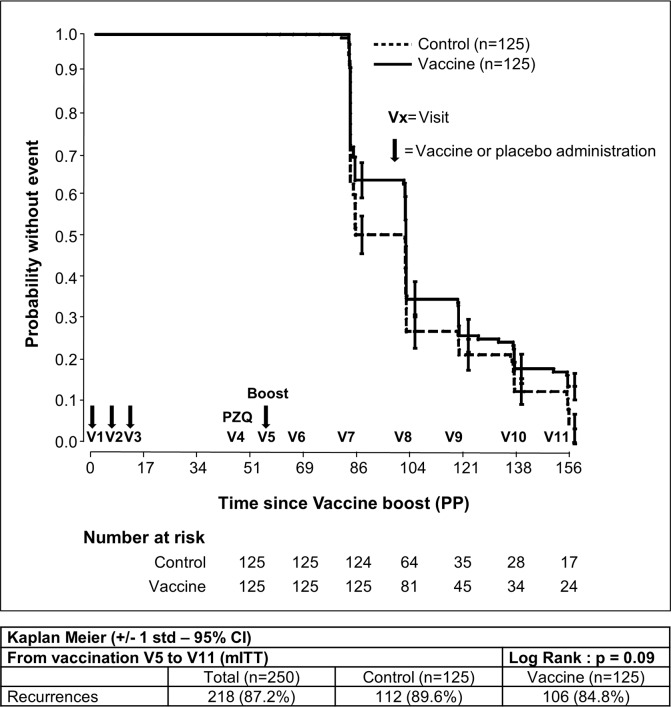
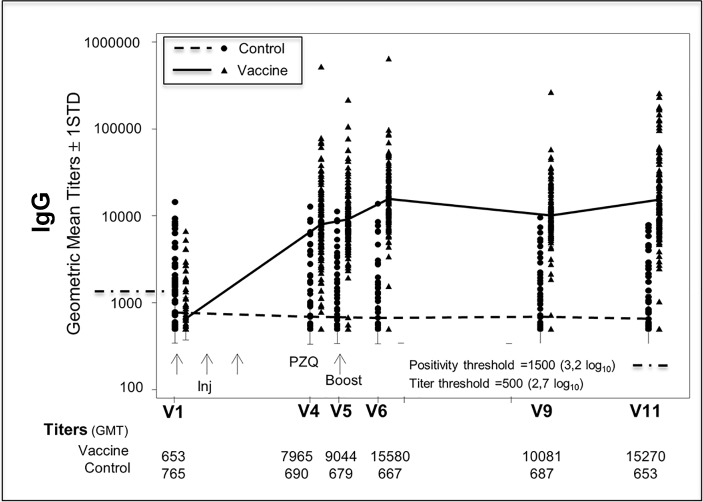
Methods and findings: After clearance of their ongoing schistosomiasis infection with two doses of PZQ, 250 children aged 6-9 years were randomized to receive three subcutaneous injections of either rSh28GST/Alhydrogel (Bilhvax group) or Alhydrogel alone (control group) at week 0 (W0), W4, and W8 and then a booster at W52 (one year after the first injection). PZQ treatment was given at W44, according to previous phase 2 results. The primary endpoint of the analysis was efficacy, evaluated as a delay of recurrence of urinary schistosomiasis, defined by a microhematuria associated with at least one living Sh egg in urine from baseline to W152. During the 152-week follow-up period, there was no difference between study arms in the incidence of serious adverse events. The median follow-up time for subjects without recurrence was 22.9 months for the Bilhvax group and 18.8 months for the control group (log-rank p = 0.27). At W152, 108 children had experienced at least one recurrence in the Bilhvax group versus 112 in the control group. Specific immunoglobulin (Ig)G1, IgG2, and IgG4, but not IgG3 or IgA titers, were increased in the vaccine group.
Conclusions: While Bilhvax was immunogenic and well tolerated by infected children, a sufficient efficacy was not reached. The lack of effect may be the result of several factors, including interference by individual PZQ treatments administered each time a child was found infected, or the chosen vaccine-injection regimen favoring blocking IgG4 rather than protective IgG3 antibodies. These observations contrasting with results obtained in experimental models will help in the design of future trials.
Trial registration: ClinicalTrials.gov NCT 00870649.
Trial registration: ClinicalTrials.gov NCT00870649.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Schistosomiasis: number of people treated worldwide in 2013. WHO. 2015;90(5):25–32. . - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
