

Novel use of a guiding catheter to relieve left main stem occlusion complicating Stamford type A aortic dissection
- PMID: 30532940
- PMCID: PMC6269265
- DOI: 10.1016/j.jccase.2012.03.012
Novel use of a guiding catheter to relieve left main stem occlusion complicating Stamford type A aortic dissection
Abstract
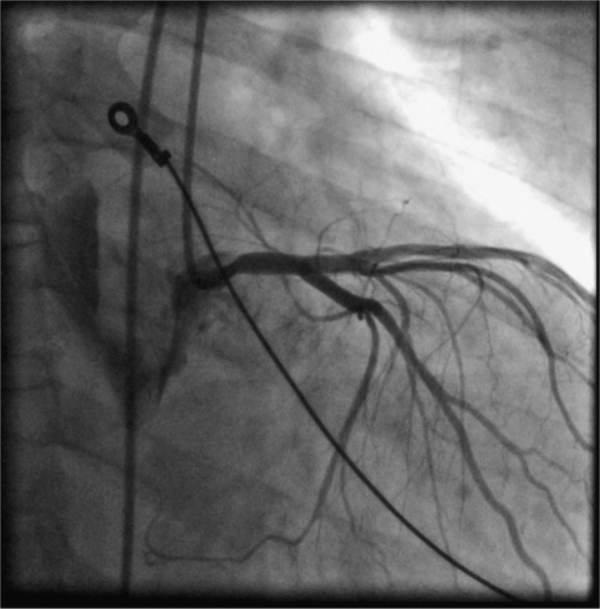
Acute ST elevation myocardial infarction occurring as a result of acute aortic dissection is a relatively rare complication with an incidence of 1-2%. However, despite this the outcome is frequently fatal. This report documents novel use of a percutaneous guiding catheter to relieve left main stem occlusion complicating Stamford type A aortic dissection, as a bridge to successful surgical treatment. A 62-year-old man presented with acute chest pain and electrocardiographic changes consistent with acute anterior myocardial infarction, and was sent for primary percutaneous coronary intervention. Angiography demonstrated an acute Stamford type A aortic dissection with associated secondary myocardial infarction caused by mechanical obstruction of the left main coronary artery by the dissection flap. Engagement of the coronary ostium with a guide catheter relieved the obstruction and allowed transfer of the patient to the operating theatre where surgery was successfully performed.
Keywords: Aortic dissection; Left main stem; Myocardial infarction.
Figures



References
-
- Kouchoukos N.T., Dougenis D. Surgery of the thoracic aorta. N Engl J Med. 1997;336:1876–1888. - PubMed
-
- Ohtani N., Kiyokawa K., Asada H., Kawatami T. Stanford type A acute dissection developing acute myocardial infarction. Jpn J Thorac Cardiovasc Surg. 2000;48:69–72. - PubMed
-
- Chan K.C., Wu D.J., Ueng K.C., Lin C.S., Tsai C.F., Chen K.S., Lin M.C., Lin C.S. Acute aortic dissection developing acute myocardial infarction diagnosed by accidentally inserting the catheters into the false lumen during catheterization: a pitfall and rare image. Jpn Heart J. 2003;44:583–585. - PubMed
-
- Spittell P.C., Spittell J.A., Jr., Joyce J.W., Tajik A.J., Edwards W.D., Schaff H.V., Stanson A.W. Clinical features and differential diagnosis of aortic dissection: experience with 236 cases (1980 through 1990) Mayo Clin Proc. 1993;68:642–645. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
