

Severe refractory asthma: current treatment options and ongoing research
- PMID: 30534175
- PMCID: PMC6284776
- DOI: 10.7573/dic.212561
Severe refractory asthma: current treatment options and ongoing research
Abstract
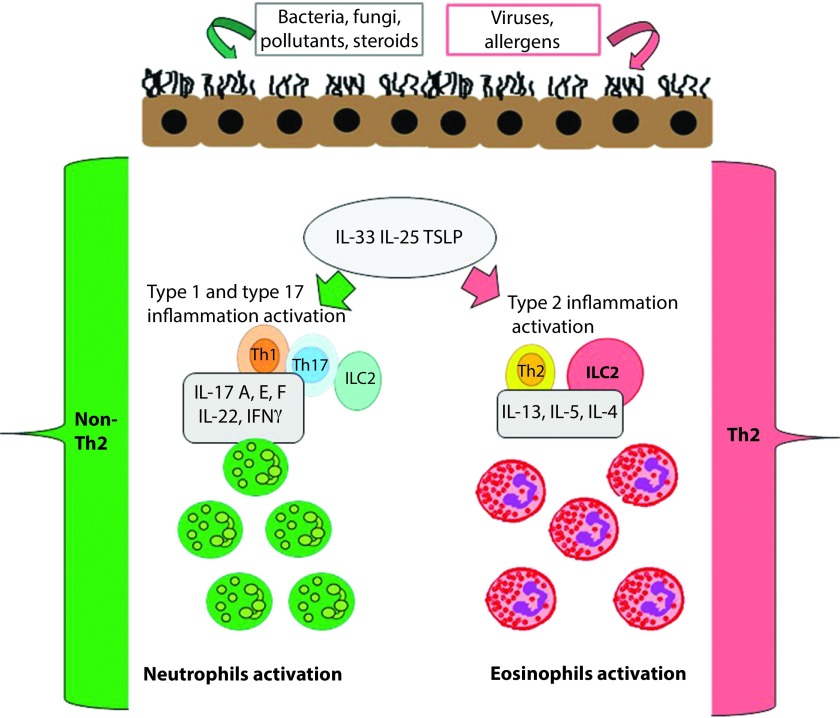
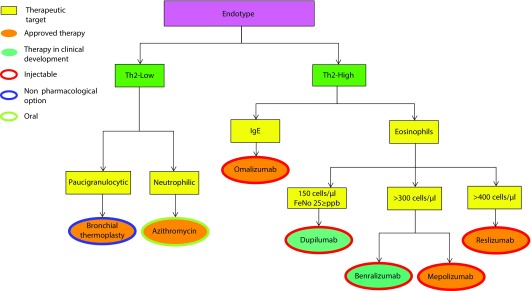
Patients with severe asthma have a greater risk of asthma-related symptoms, morbidities, and exacerbations. Moreover, healthcare costs of patients with severe refractory asthma are at least 80% higher than those with stable asthma, mainly because of a higher use of healthcare resources and chronic side effects of oral corticosteroids (OCS). The advent of new promising biologicals provides a unique therapeutic option that could achieve asthma control without OCS. However, the increasing number of available molecules poses a new challenge: the identification and selection of the most appropriate treatment. Thanks to a better understanding of the basic mechanisms of the disease and the use of predictive biomarkers, especially regarding the Th2-high endotype, it is now easier than before to tailor therapy and guide clinicians toward the most suitable therapeutic choice, thus reducing the number of uncontrolled patients and therapeutic failures. In this review, we will discuss the different biological options available for the treatment of severe refractory asthma, their mechanism of action, and the overlapping aspects of their usage in clinical practice. The availability of new molecules, specific for different molecular targets, is a key topic, especially when considering that the same targets are sometimes part of the same phenotype. The aim of this review is to help clarify these doubts, which may facilitate the clinical decision-making process and the achievement of the best possible outcomes.
Keywords: cytokines; economic burden; endotypes; eosinophils; inflammation; phenotypes.
Conflict of interest statement
Disclosure and potential conflicts of interest: Francesco Menzella participated in contracted research and clinical trials for Novartis and Sanofi, he has received lecture fees and advisory board fees from AstraZeneca, BoehringerIngelheim, Chiesi, GlaxoSmithKline, Mundipharma and Novartis. The other authors report no conflicts of interest in this work. The International Committee of Medical Journal Editors (ICMJE) Potential Conflicts of Interests form for the authors are available for download at http://www.drugsincontext.com/wp-content/uploads/2018/11/dic.212561-COI.pdf
Figures
References
-
- Chung KF, Wenzel SE, Brozek JL, et al. International ERS/ATS guidelines on definition, evaluation and treatment of severe asthma. Eur Respir J. 2014;43:343–373. http://dx.doi.org/10.1183/09031936.00202013 Erratum in: Eur Respir J . 2018;52(1). - DOI - PubMed
-
- Pakhale S, Mulpuru S, Boyd M. Optimal management of severe/refractory asthma. Clin Med Insights Circ Respir Pulm Med. 2011;5:37–47. http://dx.doi.org/10.4137/CCRPM.S5535 - DOI - PMC - PubMed
-
- Papi A, Brightling C, Pedersen SE, Reddel HK. Asthma. Lancet. 2018;391(10122):783–800. http://dx.doi.org/10.1016/S0140-6736(17)33311-1 - DOI - PubMed
-
- Ivanova JI, Bergman R, Birnbaum HG, Colice GL, Silverman RA, McLaurin K. Effect of asthma exacerbations on health care costs among asthmatic patients with moderate and severe persistent asthma. J Allergy Clin Immunol. 2012;129:1229–1235. http://dx.doi.org/10.1016/j.jaci.2012.01.039 - DOI - PubMed
-
- Heaney LG, Brightling CE, Menzies-Gow A, Stevenson M, Niven RM. Refractory asthma in the UK: cross-sectional findings from a UK multicentre registry. Thorax. 2010;65:787–794. http://dx.doi.org/10.1136/thx.2010.137414 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
